SGMC IM Resident Guide

All the clinical knowledge you need, organized and searchable on any device. A digital companion built to lighten your load and sharpen your learning throughout residency.
Contributors
If you are interested in contributing please contact the SGMC IM Resident Guide team.
Survival Guide
Intern Survival Guide
SGMC Health Internal Medicine Intern Survival Guide
Welcome! This survival guide was designed to gather resources that might make your transition to residency less complicated. It covers essential details on how inpatient work is organized, general ward management, acute and common conditions in adult medicine, and comprehensive references for each major organ system and subspecialty.
Clinical Judgment
This guidebook should not replace your clinical judgment and critical thinking. Before following any of the suggested next steps in this guide, consult with your senior residents and attending physicians.
Guide to Medicine Wards
Who to ask for help/clarification?
- Your supervising resident
- Chief Residents: Samuel Edusa, MD and Ornob Rahman, MD
- Attendings: Dr. Lamptey, Dr. Gallagher, Dr. Sobukonla, Dr. Matthew Varn, Dr. Roberta Baah-Sackey, Dwayne Mohan, MD, Rosaida Silverio-Lopez, MD, and Venkata Gandi, MD
- For outpatient questions: Dr. Bias
- Administrative questions: Ms. Dawn Marro and Ms. Tonya Moreno
Helpful Resources
- Open Evidence: AI-powered platform that aggregates and synthesizes peer-reviewed medical literature to help healthcare professionals make evidence-based decisions at the point of care through research summaries, article links, and current clinical guideline.
- UpToDate: Clinical decision support tool that provides evidence-based medical information and treatment recommendations to healthcare professionals at the point of care.
- University of Chicago House staff Guide (for critical care, heme/onc, procedures).
- Life in the Fast Lane (LITFL): Medical education website providing emergency medicine and critical care resources including clinical cases, ECG interpretation, medical mnemonics, and point-of-care learning materials for healthcare professionals
- Timeofcare.com: Website with common work-up orders for inpatient and outpatient medical conditions
- Sanford guide: Comprehensive antimicrobial therapy reference that provides healthcare professionals with evidence-based recommendations for antibiotic selection, dosing, and treatment duration for infectious diseases.
- MDCalc: Medical calculator platform that provides healthcare professionals with validated clinical decision tools, risk scores, and diagnostic calculators to support evidence-based patient care decisions.
- MKSAP: American College of Physicians' continuing medical education program that provides internal medicine questions, case studies, and educational content for board preparation and ongoing physician learning.
EPIC tips/adjustments
Prior to starting your inpatient rotation:
- Adjust your Epic print settings
- Add your favorite orders
- If not already available, create a
My Listsection to add your assigned patients. - Always right click on the patient's name and
Assign mewhen given a patient to work with. - Also send it to your list by clicking
Send toand thenMy list. - You should also add the patient to the
Night Medicine Residency list.
Example of how to setup your Epic Tabs
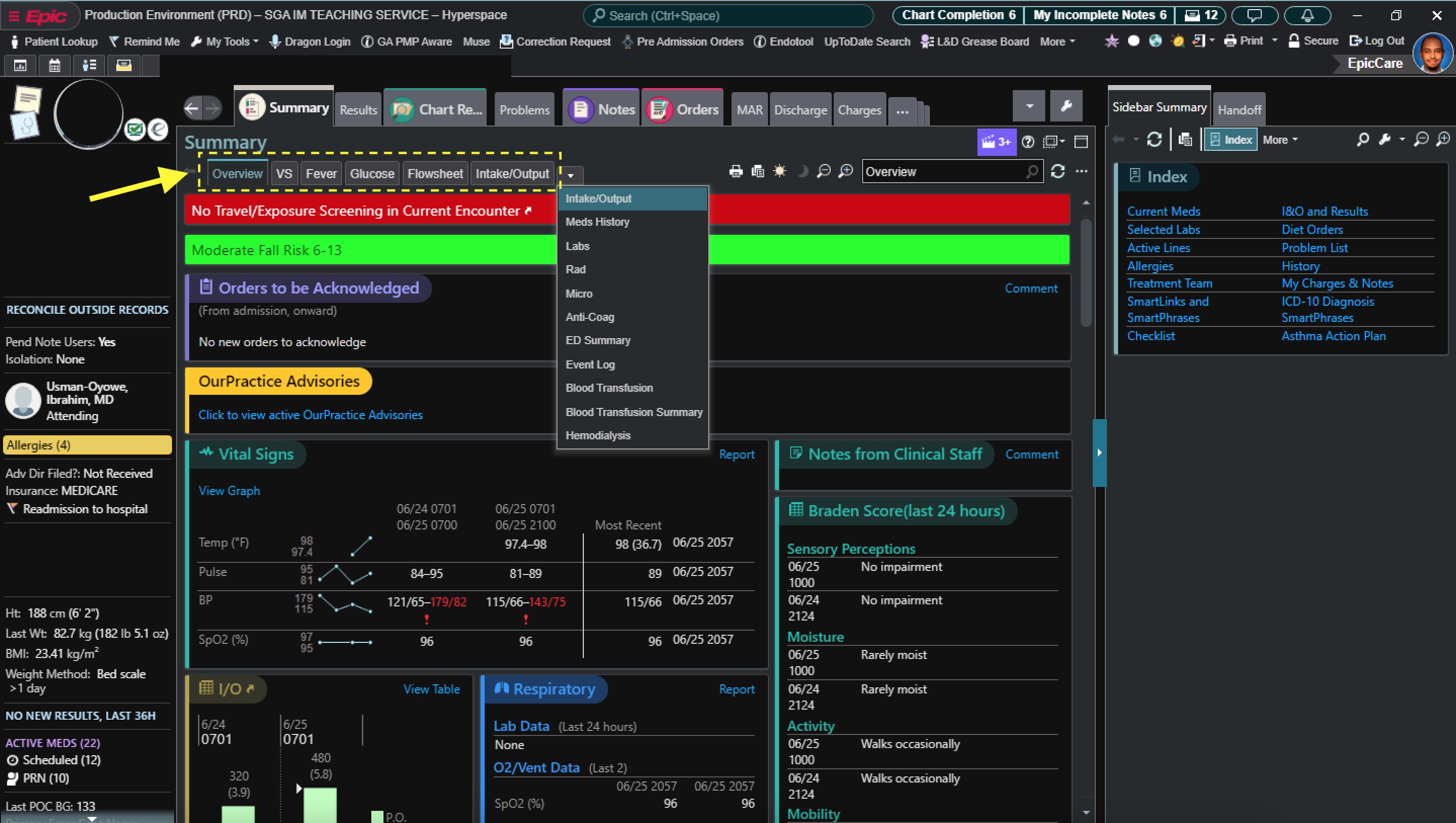
Include on your printed handoff the following items by right clicking on your My list, clicking Properties, and below at Selected columns, have the following:
- Room/Bed
- Patient Name
- Age/Gender
- Blank column
This should print the following:
- Patient's name and room number
- MRN, age, weight, allergies, admission days, date of admission, code status, attending, PCP
- Empty summary box
- Last recorded vital signs with lowest and highest value in the last 24 hours including temperature, pulse, respirations, blood pressure, and FiO2%
- I/O for the last 3 completed shifts, quick overview of CBC (it won't include WBC), chemistry, electrolytes (it won't include glucose) and medications
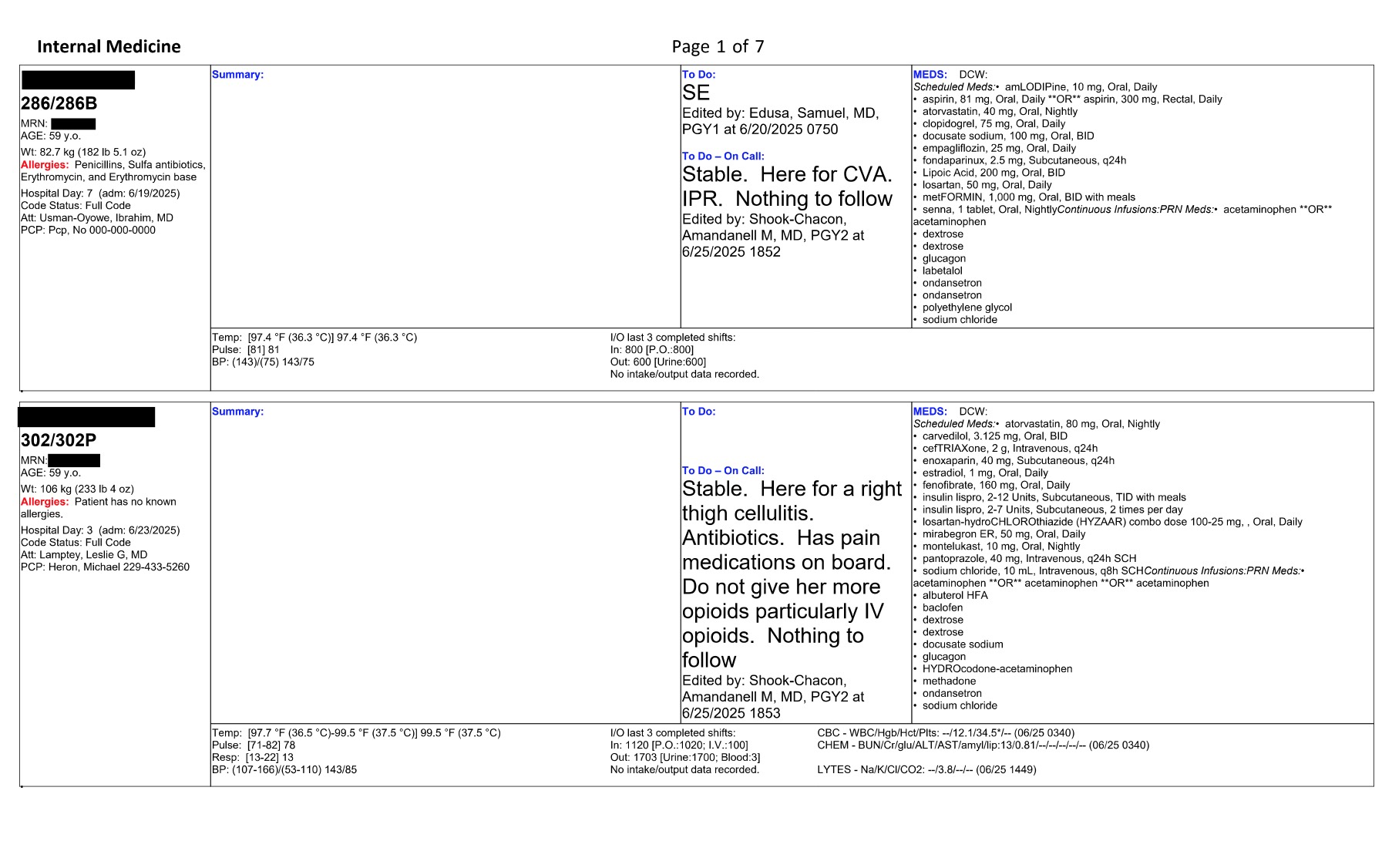
Example of a handoff
To add to your favorite orders:
-
Go to
Ordersand on the right-hand search box, there is aNewbutton, click on it and it will allow you to search for physicians' favorites. i.e. If you search forAgrawalinSearch order sets and panels by user, you will findadmission orders, anddischarge ordertemplates. You can add them to your favorites and select or unselect as you work with your admissions. -
For a full report of laboratory results, in the summary section, add
Labs. This will simplify your view of completed labs to date in the present admission.
Getting into action...
To have a successful rotation, it is recommended that you:
- Apply good teamwork
- Proper communication
- Call your consults early
- Stay proactive, and remain available to your patient and team's needs.
Other Important Tips
- Be nice to everyone (nurses, RTs, consultants, ED team, peers). Professionalism is key.
- Follow your chain of communication.
- Set expectations upfront with your senior resident/attending (i.e. how often should interns check in with seniors, etc.).
- Always ask your senior resident if you are unsure of something.
- Important things to inform your senior resident include changes in vitals (fever, tachycardia, hypotension/hypertension), hypoxemia or increasing O2 requirements, new altered mental status, significant lab abnormalities, or other significant change in patient status.
- Return calls or secure chat messages in a timely manner (<10 min). Triaging pages in order of importance is vital to good patient care.
- Update the nurses after rounds with the plan of care for the day.
- When entering NPO order, write the reason for NPO in the comments section.
- When pt is NPO, make sure to adjust insulin as needed (see DM section). Talk to your senior for help.
- If pt is NPO for several days, consider maintenance IF fluids (MVIF) (eg, D5NS at 75 ml/hr) vs enteral nutrition via NGT.
- If pt is NPO overnight for an AM test/procedure, no need to give MIVF.
- When ordering IV antibiotics, always think about age, kidney function, and indication. If you're unclear on a dose - call pharmacy, they will help you. Also check previous
Microsection for past positive cultures and susceptibility.
Before you start wards:
- Meet with your teammates and review your inpatient schedule. Your schedule will be provided prior to the start of your rotation. Chief residents arrange long call vs short call days along with days off.
- Ensure your teammates have your contact number. Remember to use Qliq when messaging about patients.
- Message your supervising resident. Let him/her know you are excited to start working in this rotation with them and inform them of your clinic days. They may message you and your co-intern together in a common group text. They may or may not include the attending as well.
- Also remember, you are a team. If one intern is running a little late, help your co-intern and reach out. If you move somewhere in rounds, communicate, and let your co-intern/resident know where you are.
- If you must give information to the resident or attending about your co-intern's patient, give your co-intern a head up beforehand when possible.
- Review the calendar days for noon report and mark them early so you can start thinking of interesting cases to present and can prepare with enough time.
- Get sign out from the current inpatient team and know what patients you will be taking over. This usually happens the day prior to starting your rotation. Your patients are assigned by your supervising resident or attending.
Layout of a full day in wards (This layout may vary depending on team or rotation changes, please be flexible and open to)
Preparing for rounds
-
(1) Arrive between 5:30 – 5:45 AM. You might need to adjust your arrival time prior to or after getting used to the system and flow of work.
-
(2) 5:30-6:30 AM. Pre-chart. Pre-charting is the practice of reviewing the patient's record to get a better understanding of the patient's overall health status and the plan of care.
Tip
When pre-charting, here is a summary of the sections that you can access in EPIC:
- Chart Review: To see previous notes, labs, images…
- Summary: Labs, radiology, micro, cardiology (to see EKG), reconcile (to see what meds they had at home).
If you notice labs that need to be ordered or tests that should be done early or pertinent/urgent abnormalities that need to be addressed suggest before rounds.
Read the ED notes to get an idea of what's going on with the patient. If the patient has already been admitted, review H&P and consult notes.
Dr. Brown, ID attending, in his ID expectations provides an excellent detailed layout on how to thoroughly review a chart. You can access it in the Internal Medicine Residency General Guide.
-
(3) 6:30-7:00 AM Go talk to night nurses before shift change at 7:00 AM. Check in with them and verify if anything happened overnight.
-
(4) 7:00 AM Get sign-out in the GME area. This might be slightly delayed depending on the night team. If you're signed out a patient as being sick - see them/check vitals/labs FIRST. You can message your senior urgently if you see them and the patient has concerning findings.
-
(5) 7:15-8:15 Go see the old and new patients. Return to the GME area and start writing notes. In the subjective portion of the notes, include overnight events, patient's overall status, complaints.
-
(6) Be ready for rounds by 8:30-9:00 AM. Attendings will usually come to GME. Some attendings would want to see you directly in 3W/4W/Tower. Clarify with your senior the location where rounds will start and be on time.
-For some attendings rounds will start by seeing patients that are potential discharges first. Some attendings would want to see very sick patients first. Try not to discharge or transfer before rounds unless the attending tells you to do so. - Anticipated discharges still need an order for discharge on the day of discharge. - If you are asked to transfer a patient, under
Ordersplace a new order by typing Transfer patient. Then select where you would want to transfer the patient. To finalize, go to theTransfertab and decide what orders will continue upon transfer. - Anticipated discharges still need an order for discharge on the day of discharge.
During rounds
- Present patients.
Note
Example of presentations
- Attending A: PMH, CC, HPI, physical exam, pertinent labs, imaging, assessment, and plan per problem.
- Attending B: Why is the patient here? What are we doing for the patient? Why can't the patient go home today?
- Attending C: Subjective (PMH, CC, HPI), Objective (vitals, labs, images, physical exam), Assessment and plan.
-
Get orders to put in and confirm assessment and plan if necessary. Have pen and paper to write down plan. If unclear, verify with resident/attending. Some orders are critical and may require immediate attention. If so, place them via Haiku on your phone, but know that some consults and orders cannot be placed via Haiku. If unable to use Haiku, try to find a computer station close by, and enter them quickly.
-
Rounds end around 11:30 AM-12:00 PM. If participating in half-days at the clinic, make sure your resident/attending knows where you stand with note status and patient care. Before leaving for the clinic, do a brief sign-out to the resident and inform labs/results to follow-up on.
-
After rounds, at 12:15, be ready for noon report/lectures. If you are presenting, let your supervising resident and team know. You will pick a patient for the report days prior to prepare well. This case should be preferably a new admission that you learned a lot from or a patient with an interesting diagnosis. It could also be a “bread-and-butter” case, and if possible, provide a good teaching point at the end of your presentation.
After rounds/noon report:
- Place orders
- Write notes
- Some attendings will review the plan of care and perform a second round.
- You may need to check on sick patients again.
End of the day:
- All notes finished.
- Relevant events that occurred during the day and must be informed right away include pertinent notifications from nurses, changes in vitals, pertinent labs that needed replacements, important orders that were put in, new imaging findings or updates from consultants.
- Review consult recommendations especially if patient is surgical. If surgery is anticipated in the AM, make sure NPO orders are in starting midnight. If needed, hold anticoagulation/DVT prophylaxis, and make sure PT/INR, aPTT, type and screen is ordered if applicable. If patients receive night insulin and they are to be NPO, consider decreasing dose or holding for that evening to avoid hypoglycemic events.
- Call family and update on plan of care.
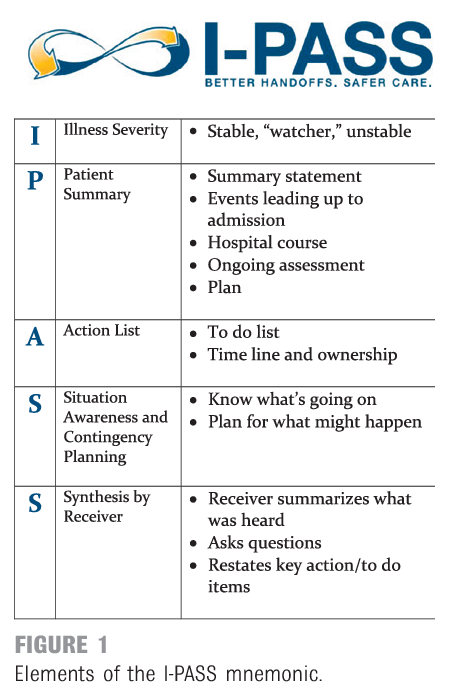
- Get ready to sign-out with the cross-coverage team. Update the Night Medicine residency list. Use IPASS (see figure below) for your sign-out.
If you are short call, you may leave at 3:00 PM if all your work is done and you have been cleared to go by your senior. Prior to leaving, you are responsible for signing out to the cross-coverage team. Remember to forward any Qliq messages and notifications to the cross-coverage team or the night team if received after 7:00 PM.
If you are long call, you are responsible for printing the list for all teams for start of the day census. You will put in the administrative office by GME, along with the admission sheet from the night before. You will be responsible for receiving all the admission calls and receive floor calls for all teams. You should also have available an admission sheet documenting the admissions your team receives during the day. You will be responsible for both call phones. (229-561-4596/229-5614597). You will stay to provide sign-out to the night team. Your admission time ends at 6:15 PM. If you receive an admission after, you might save it for the night team. Still, obtain a full report from the ED so you can provide the admission details to the night team.
See below an acronym you may use during sign-out. Also remember to highlight CODE STATUS.
Layout of a full day in wards, in summary
- Pre-chart.
- Get sign-out on patients from covering night team at 7:00 AM. You may get signed out overnight admissions depending on where you are in the call cycle.
- See all patients (unless pre-determined with your team).
- Replete electrolytes, order blood prn.
- Start (ideally finish!) progress notes.
- Be ready for rounds from 8:30-9:00 am to 12 pm.
- Afternoons are typically for catching up on tasks, finishing notes.
- Sign-out to the cross-cover or night float team when your senior tells you it's okay.
- Contact family and update on plan.
- Night float typically begins cross-cover at 7pm – confirm with your senior.
Tips/Common Questions
- If a patient is admitted for hypoxia, know the O2 Sat, if they have blood gases, what are their values? How would you interpret them? How much oxygen is he on?
- When typing a note, it's better to be precise with important information.
- Hypocalcemia? Always look for albumin and correct.
- Hyponatremia? Correct if diabetic and hyperglycemia is present.
- DKA when is it resolved? When the anion gap closes.
- Patient with SVT and stable first thing to do: Vagal maneuvers.
- On the days you have clinic, you might need to be more proactive.
- Avoiding arrhythmias is worth it. Use the "2–3–4–9" rule to remember the desired levels of magnesium, phosphorous, potassium, and calcium, respectively.
-
Know the seven Ps for each of your patients: Problems, Progress, Pain, PO (oral intake), Pee-Pee, Poop, and Physical condition.
Problems: refers to the problem list you are addressing for the patient (i.e., why and how the patient came to be under your care) and what you are doing for each with respect to either diagnosis or treatment.Progress: refers to the events in the past twenty-four hours that have happened positively or negatively to your patient. Progress is what the team will want to hear about every day.Pain: Assess your patient's pain and adjust medications so the patient is reasonably comfortable.PO: Know how your patient is getting nutrition and how far you can advance his or her diet. Patients should be NPO (taking nothing by mouth) post-surgery until they have bowel sounds; then clear liquids may be started, and continued until the patients pass flatus, when solids may be tried. Do not be afraid to go slowly or take a step back. If a patient is not taking food by mouth, note the nutritional route or the reason for withholding oral nutrition; if he or she is eating, know the type of diet (e.g., clear liquid, dysphagia ground, diabetic, low salt, regular). Know your patients' urine output and if it is adequate (i.e., at least 30 mL/hour; perhaps less for children and the elderly) and the route (i.e., via catheter or naturally).Pee: If a patient is off a patient-controlled analgesic (PCA) or other, more-invasive pain control (e.g., an epidural catheter) as well as able to sit on a bedpan or use a urinal, get that foley catheter out. When removing a foley catheter, be sure to write for bladder scan after six hours if the patient has not urinated, and to replace the Foley catheter if the bladder scan is more than 350 mL.Poop: Assess the number of days since the patient's last bowel movement so you know how to adjust bowel care.Physical condition: Understand the patient's physical condition and progress with physical, occupational, and speech therapy as well as all other consults required to aid in the management of the patient's case.
Admissions
- You will get a call from the ER doctor. While on the call take notes on name, location, PMH, CC, what has been done for the patient, orders they want you to follow up on, and why the patient is being admitted. If possible, do a quick review of the chart while on the call and ask questions.
- Once you have the patient localized on Epic, assign yourself to the patient by right clicking on the patient and selecting
Assign me. Double click on the patient and open the chart. Go to the Summary tab. In the Comment section, enter the dot phrase.RESPTto include the call phone contact disclaimer. Send the patient to your team’s list and the night medicine list. - Inform your resident. Ask if you should admit right away or go see the patient, evaluate, and then if appropriate put a general admission order to either Inpatient or Observation. This will likely depend on severity. Ask the resident where to admit the patient to. In most cases, you will admit to inpatient if care/hospital stay is predicted for at least 2 midnights. If this patient is expected to stay less than 2 midnights (diagnostic examples: TIA, CVA rule out, syncope, other), you may place in observation status. Talk with your supervising resident and put overall admission orders together.
- When you go see the patient, get HPI, thorough medical history and physical exam, think of assessment and plan, think of additional orders. If family is present, make sure to obtain contact number and add information to chart if not available before. Address CODE STATUS for all your admissions. Discuss the patient with your resident. Work on your H&P note, and then be ready to discuss and present to your attending.
- The flow of admissions may vary depending on teams and attendings.
Admission Checklist
- Assign yourself to the patient and add to your patient list and night medicine list.
- Look at admitting diagnosis and vitals.
-
Chart review:
- Look at ED notes and interventions (you can find ED clinical summary under summary tab which tells you when they got fluids etc.)
- Look at previous discharge summaries
- Look at results (labs/imaging)
-
Place basic orders. Observation status vs inpatient.
-
Go and see pt and obtain HPI
- If a patient looks acutely ill, call senior.
- Obtain HPI, PMHx, etc. Do physical exam.
- Reconcile med list / Order appropriate home meds – this includes calling patient's pharmacy and confirming meds are correct- if theirs is closed, see if there is a 24hr one available
- Confirm code status (place order)
-
Staff the patient / discuss with senior
-
Place admission orders. (Usually General Adult Admission order set, but look! There are often disease-specific order sets available).
- Hold diet until talk to pt and you are sure that no interventions that might require NPO
- Order DVT ppx – make sure plts >50k on labs and no other contraindications, also choose correct ppx for CrCl (<30 heparin, otherwise Lovenox— which is much better since it’s once daily vs. two- three times daily. and requires no surgical interventions). You may use Xarelto if patient is stable, tolerating PO and with no potential surgical dx.
IMPORTANT: All admission orders should include the following PRN meds:
- Tylenol 325-650mg q4h prn for mild pain or headache (2g max in cirrhosis). You can put in comments to "call for fever." Unless liver disease, high LFTs.
- PRN for constipation (i.e. Miralax 1 packet once daily prn (or a bowel regimen of your choosing)).
-
Sign and hold orders if still in ED.
-
Final Orders
- Make sure home meds are correct
- Place any additional orders discussed in staffing
- Confirm that orders match the written plan
-
Finish writing H&P
Progress Notes
- Subjective: a quick outline of important events in the last 24 hours, issues the nursing staff has mentioned that the patient may not have, any updates on their condition that the patient mentions to you (worsening nausea, improved pain)
- Vitals: they are vital and must include numbers in a range of lows and highs over the last 24 hours; afebrile is not a vital sign.
- I/O’s: include totals in and out as well as specifics (what amount out was urine, how much was stool, how much was vomitus)
- Meds: copied into the note and updated daily. This is a great time to make sure medications are renewed and adjusted appropriately
- Physical Exam: system based, highlighting pertinent data/findings on examination. You may include media pictures for skin findings.
- Labs/Imaging/EKG: include daily labs, pending or completed culture results including sensitivities, any new radiographic studies, EKG if applicable performed since the last note you wrote.
- Before your Assessment/Plan you may include a quick, one-liner including the patient’s age, sex and primary problems for current presentation.
- Assessment: Describes the diagnoses, attributable cause and your subjective/objective data to support the diagnosis.
-
Plan: List this out by the issues
- Each problem should be listed separately along with what you plan to do about it that day and what was done about it the day before
- Any problem which has resolved in the last 24 hours should be listed one last time to acknowledge its resolution and then can be dropped from the list If you don’t know the specific plan on an issue, you may write, to be further discussed with team – an addendum note can always be completed later
-
Be sure to mention prophylaxis daily (Nexium, SQ heparin, SCD’s) in every note
- Always end your note with CODE status
- Document family discussions
Discharges
- Daily discussions with your seniors/attendings and social worker/case manager/nurses/families are crucial for a proper discharge process. It is imperative that you update social workers on each floor on discharge planning. Review PT/OT notes for placement recommendations and provide prompt instructions to social workers/nurses along with family members. Placement at rehabilitation facilities varies depending on physical needs and are sometimes subject to insurance approval.
- Placement considerations:
- (1) SNF: Skilled nursing facility. Examples of patient needs: Prolonged IV antibiotic course, ongoing 24-hour nursing care, patients that live in SNF already, unable to care for self if living alone. This provides a more medical-like environment than assisted living facilities.
- (2) SB: Swing-bed. Examples of patient needs: Need for rehabilitation in hospital-like facility, need for strength recovery prior to discharge home, post-surgical patients.
- (3) Assisted living facility: Examples of patient needs: Patients are independent with good ADLs tolerance but live in a facility with household similar accommodations.
- (4) IPR: Inpatient rehabilitation facility. Examples of patient needs: Patients with more intense rehabilitation needs, that are able to participate actively in therapy. At times, they have medical conditions that require monitoring/optimization. This is in-hospital rehabilitation.
- (5) Home with home health +/- PT/OT. Examples of patient needs: Patients that will require visits for at home assistance with monitoring of medical conditions or PT/OT. They typically require less intense rehabilitation measures.
- (6) Hospice: At home or facility. Recommended after a Palliative Care consult.
Discharge Checklist
- Go to
discharge navigator. -
Must do on each patient:
- Med Rec: THIS IS ONE OF THE MOST IMPORTANT THINGS WE DO so it should be done correctly. Ask your senior to help you or check it once you are done
- Follow up Providers: It is better to schedule follow-ups then rely on your patient to do so
- PCP communication: Underrated but so important. Ideally PCP should be called every hospital stay.
- Pt hospital summary: Use this instead of D/C instructions because it'll go on the top of the AVS instead of bottom. You can put stuff in D/C instructions over the course of their stay as it is a working document of sorts (unlike the pt summ) and then just copy and paste into pt summary on day of discharge
- D/C Summary: Remember busy PCPs are reading these so keep it as concise as possible. Be sure to document changes in meds, pending labs, things you want them to do.
- Preview AVS then sign AVS/CoC
To Call a consult
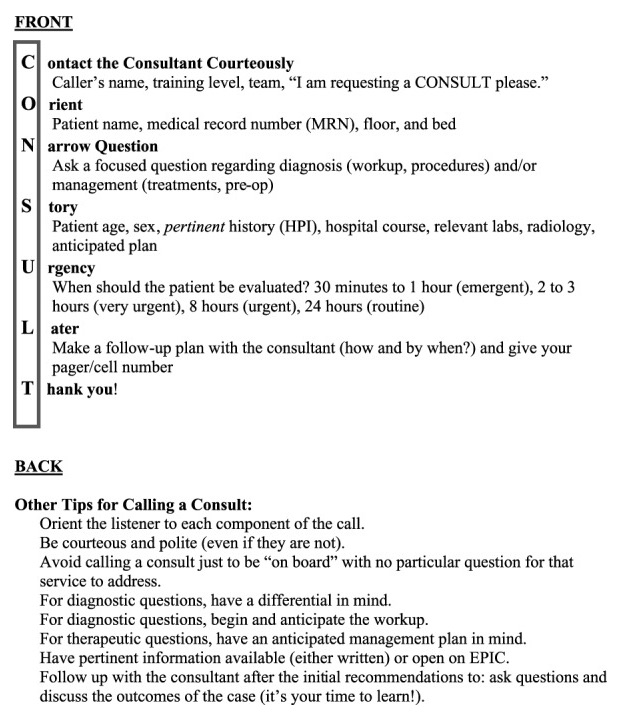
Introduce yourself, PGY- year, the attending that you are working with and the service that you are on. Say the patient’s name and room number. Give brief PMH and reason for the consult. A mnemonic is included below to summarize the steps and help make your interaction easier. You should only call consults after 8 weeks of training and in the presence of your senior. Once you have finalized your consult call, DON’T FORGET TO PLACE THE CONSULT ORDER ON EPIC!!!
Significant Event Notes & Hospital Courses
- You should write a significant event note or progress note anytime you make a significant intervention in patient care, anytime you evaluate a patient (on nights), anytime there is a Code Blue/Rapid Response called (senior resident can do this as well).
- If present on the note, try to update the hospital course so your colleagues are up to date. This will make your d/c summary so much easier/quicker. This documentation should be CONCISE, and include important information for an outpatient provider to know or for an ED/inpatient provider to know if they are a frequent flyer (i.e. echo results, important changes in long term care).
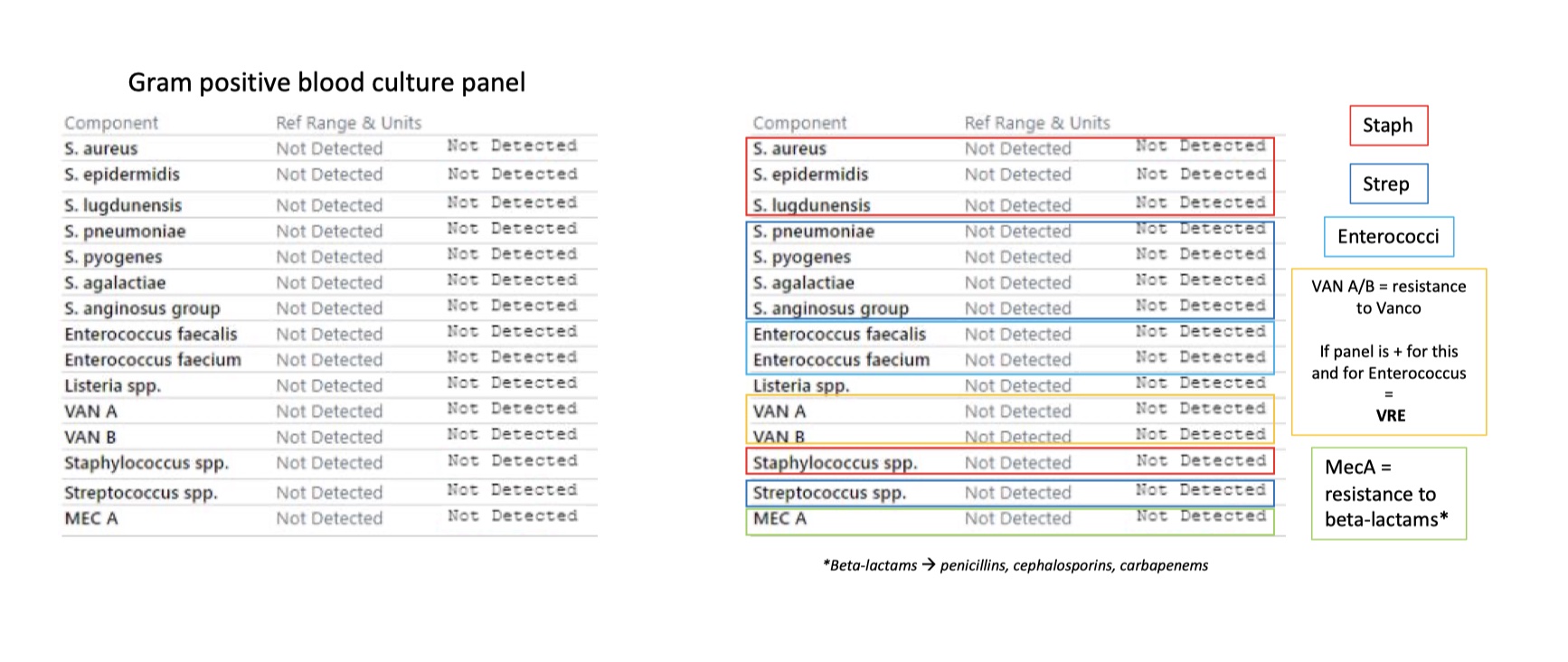
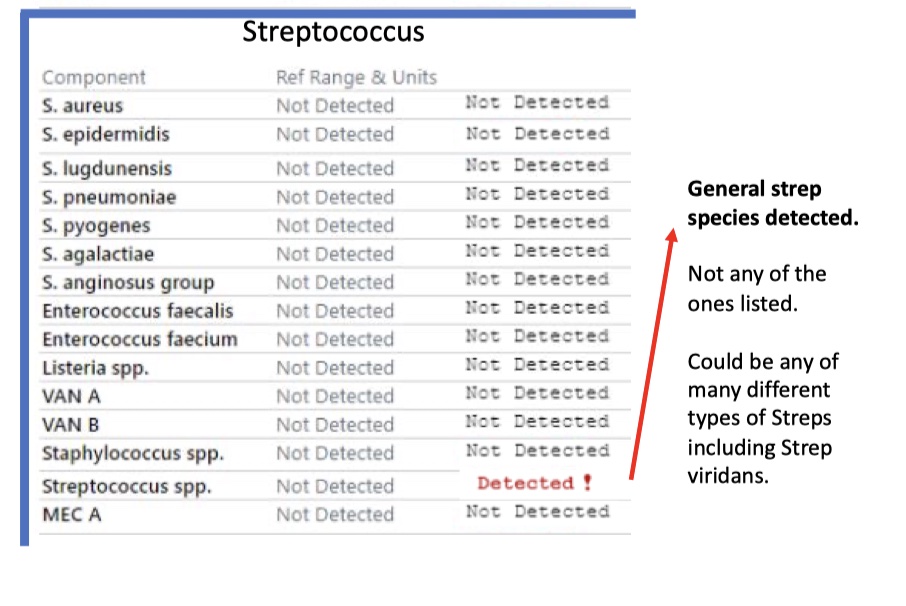
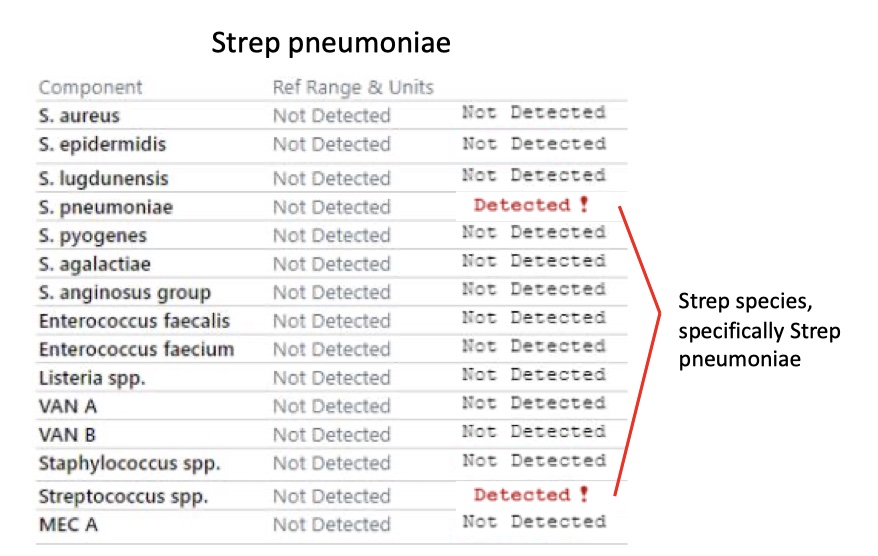
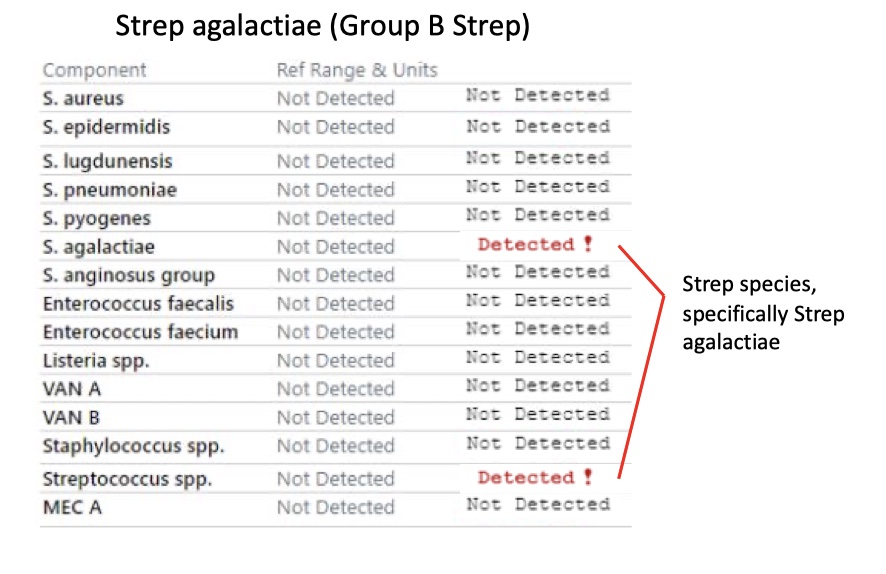
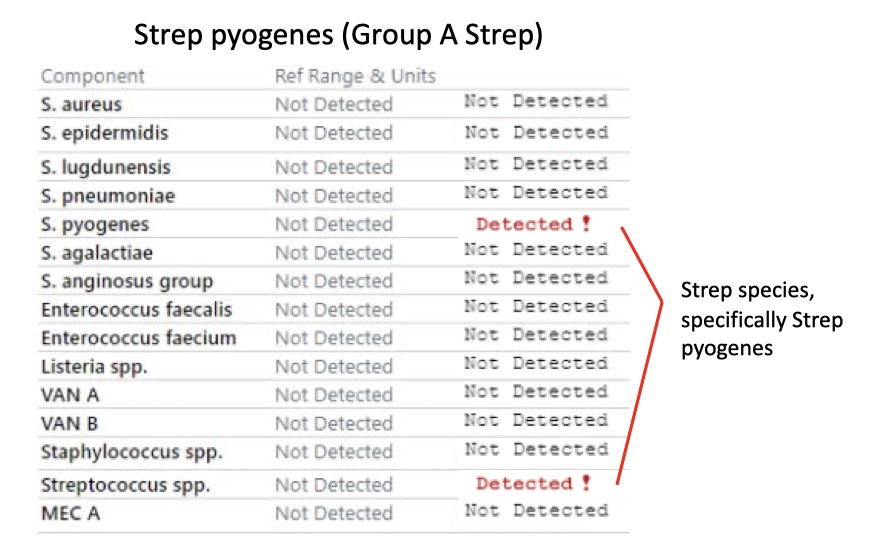
Blood Culture Interpretation
Gram positive blood culture panel interpretations
Gram positive blood culture panel
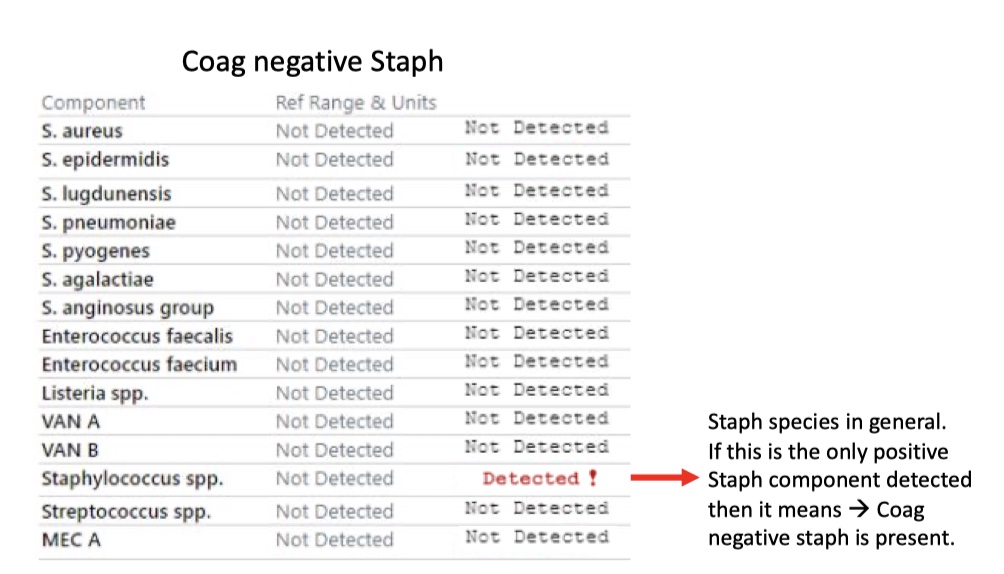
Coag negative Staph
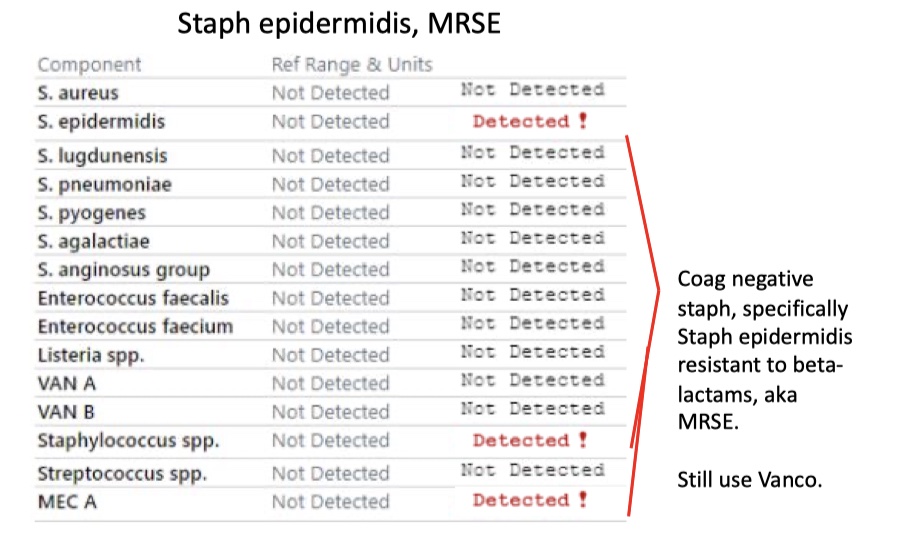
Staph epidermidis, MRSE
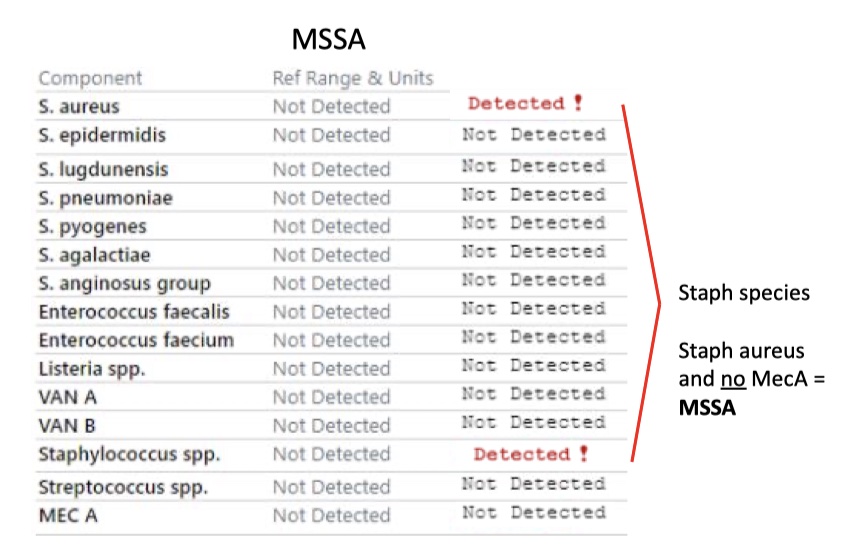
MSSA
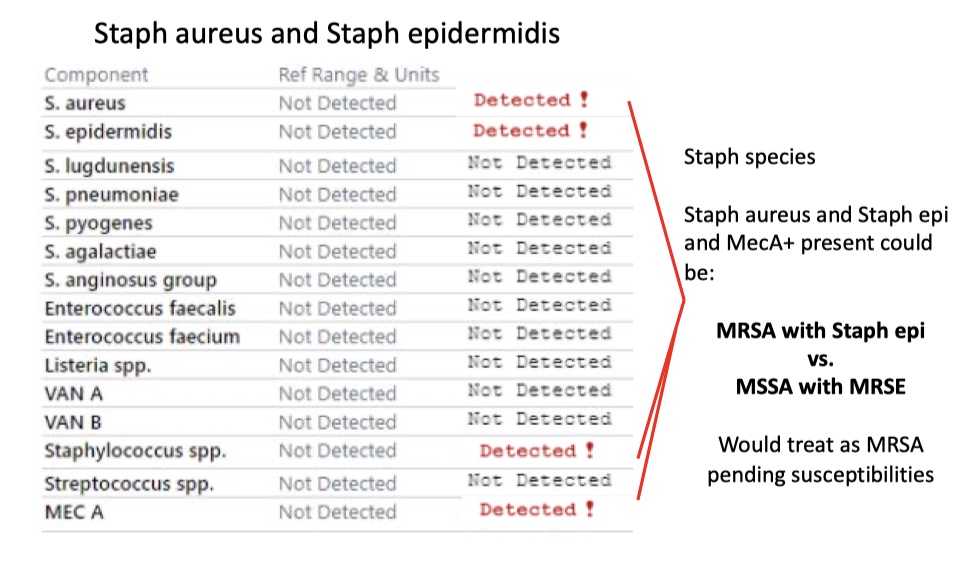
Staph aureus and Staph epidermidis
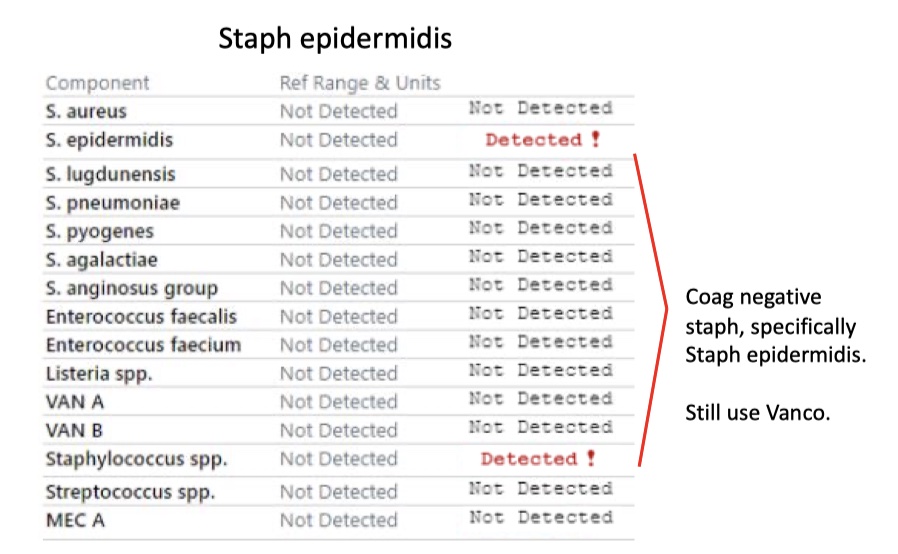
Staph epidermidis
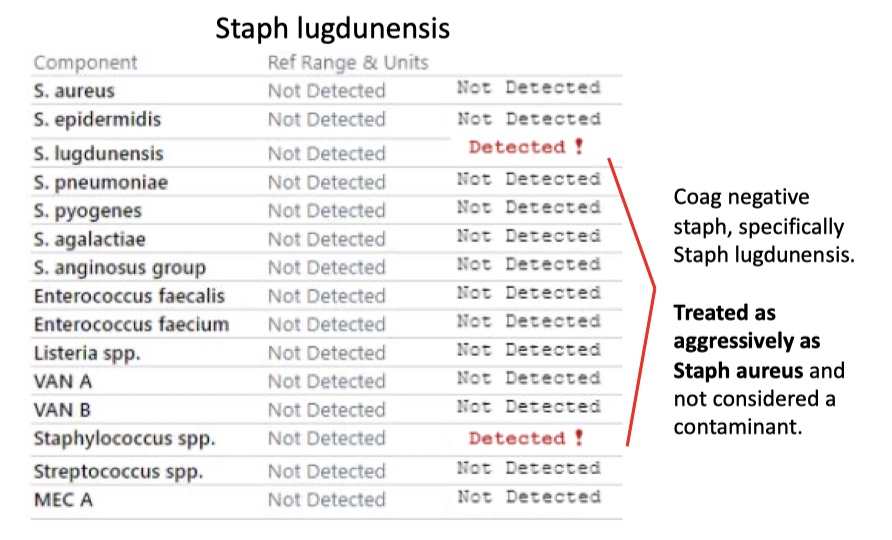
Staph lugdunensis
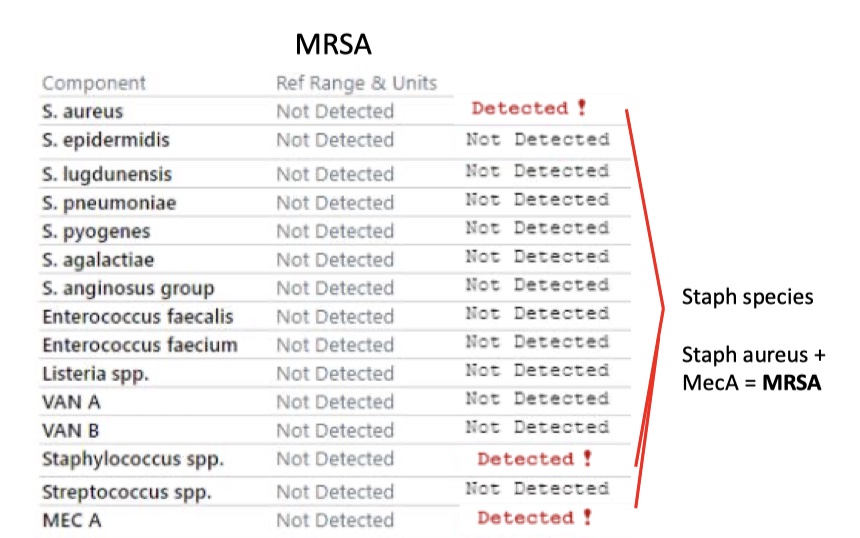
MRSA
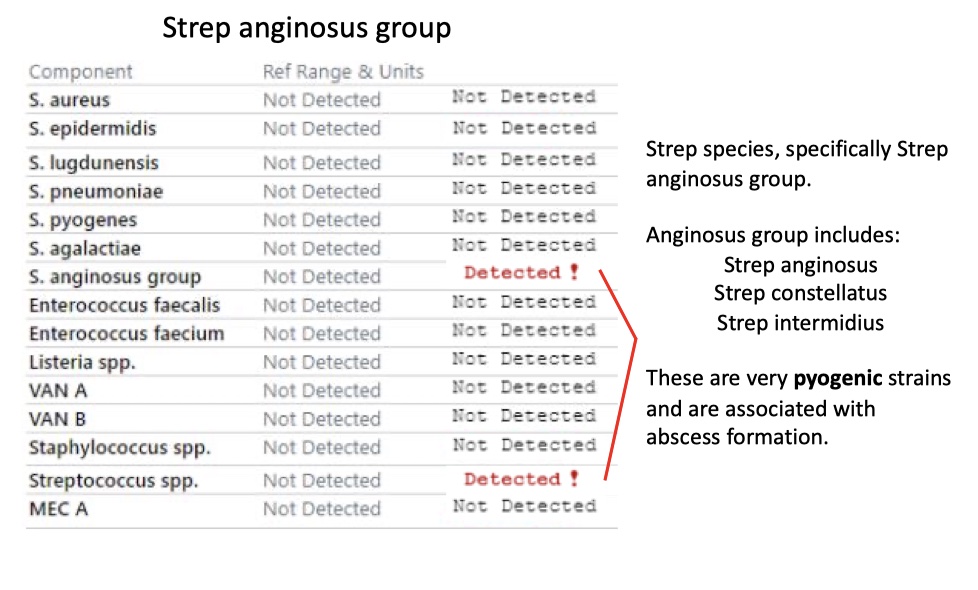
Streptococcus
Strep pneumoniae
Strep agalactiae (Group B Strep)
Strep pyogenes (Group A Strep)
Strep anginosus group
Disclaimer
Always verify with your superiors before taking action based on this guide. The information is intended to help, but not to dictate your course of work. Always use critical judgment and your clinical knowledge skills. This guide will be constantly revised and updated according to evidence-based medicine.
Ward Management Essentials
Things to Know About your Patients
- Old EKGs: Most adult patients will have an EKG, and it’s a good idea to know what it looks like - from a medication standpoint, the QTc is the most important thing to look at because it may affect your choices. Always go to
Care Everywhereto review outside records if unable to find data in chart review. - Prior echocardiogram: What was their most recent ejection fraction? Any severe valvular disease?
- Creatinine: Normal, or do they have CKD?
- Hemoglobin: baseline, most recent
Electrolyte Replacement
Potassium
Rule of thumb: 10 mEq generally increases level by 0.1 (0.2 in renal disease/CKD)
- If the gut works, use it (IV burns and you have to give it slow)
- PO can be pill or packet – let RN and patient decide (pill is large, sometimes hard to swallow)
- Max PO is 40 mEq q3-4 hrs or IV 10 mEq q1h (or 20 mEq through CVC)
- Replace if <3.4 or so in healthy pt, <4.0 in cardiac pt
- If <2.9, would consider tele and repeating lab after replacement
- Check Mag: if low, will not absorb K properly and need to replete
Magnesium
- Oral tablets (400-800 mg/24 hrs or IV 1-4g depending on severity)
- Replace if <1.6 or so in healthy pt, <2 in cardiac pt
Phosphorus
- Oral (K phos neutral tablet or Phos-nak solution) or IV (potassium or sodium phosphate)
- Replace orally unless cannot take PO. IV phos is dangerous (can cause arrhythmias and renal failure) and is run really slowly, like 4-12 hours
- Replace if <2 and look on uptodate or ask pharmacy for specific dosing (typically 1-1.3 mmol/kg divided in 3-4 doses in 24 hrs)
- Be cautious in severe renal dysfunction (check and see if pt is on a phosphate binder, calcium acetate or Phoslo).
Electrolyte Derangements
Hypoglycemia
There is a hypoglycemia protocol that you can order:
- If ≤70 and pt A&O, have RN give orange juice/crackers and recheck in 20 min
- If ≤70 and not alert and oriented or cannot take PO/swallow, give 1 amp of D50. If no IV access for whatever reason, then can give 1 mg of glucagon SQ or IM. Recheck BG every 20 min or so
Hyperglycemia
Typically hold oral anti-diabetic medications once admitted. Order basal-bolus regimen (recommended based on RABBIT 2 trial) or sliding scale insulin alone (SSI).
- If they don't have diabetes DO NOT give them insulin unless necessary. People have stress-induced hyperglycemia in hospital so it is normal to see slightly high glucose in even the healthiest of patients.
- If BS greater than the limit of the sliding scale, can give a one-time Humalog dose (only if >1hr after last insulin was given) and then either adjust long-acting insulin or sliding scale or sign out to daytime to do so.
- Review sliding scale requirements every day in glucose tab (under summary tab) and use this to guide long-acting dosage and/or add on standing short-acting. Talk to senior about this as it is not intuitive!
Hyperkalemia
- Make sure it is real (ie, not a hemolyzed sample)
- 3 typical mechanisms causing hyperK: increased K intake (meds, IVF, TPN, pRBCc), transcellular K shifts (like in rhabdo), or impaired K excretion (AKI, CKD, RAAS inhibition, aldosterone antagonism)
- There is not a well-defined treatment threshold but typically give acute treatment if ≥6+EKG changes or ≥6.5 regardless of EKG changes. Most people typically start treating around 6.
- K 5.5 – 5.9: review med list (ACE-i/ARBs?, K- sparing diuretics), r/o urinary obstruction (via bladder scan), and check glucose as hyperglycemia alone can cause hyperkalemia. Recheck in 6-8 hrs to see if up-trending.
- If EKG changes present (peaked T waves, widening QRS), place pt on cardiac monitor and give 1 g IV calcium gluconate over 15-60 min (in addition to treatment below). Then recheck EKG and re-dose calcium if changes still present (keep doing this as necessary).
- Get rid of K through urine if you can (i.e patient is not anuric).
- If patient is anuric, then use Kayexalate (30 g) but ensure they have normal bowel function and not a "sick bowel" (GI bleed, obstruction, recent surgery), as there is risk of colonic necrosis.
Acute therapies:
- An order set is available on Epic by searching
Hyperkalemiain the Orders tab. You will have various treatment options including insulin + dextrose, albuterol, sodium zirconium - Lokelma, and others. - Loop diuretics and saline (can use one or the other or both as they increase Na delivery to ENac channels causing K excretion). Another rational for saline is you don't want to make a euvolemic patient hypovolemic. Don't give saline if hypervolemic.
- Insulin + Dextrose but omit dextrose if patient already hyperglycemia. Be aware of hypoglycemia, especially in CKD pts. Recheck glucose q30 min-1 hr x 2-4 times
- Less common: Albuterol 10-20 g!! (typical dose is 2.5 g), Kayexelate, if anuric as stated above
- As stated above, don't forget to r/o urinary obstruction and hyperglycemia
Transfusion Guidelines
- Cryoprecipitate, FFP should only be ordered in certain circumstances on discussion with team.
- Note: These have changed due to the blood transfusion shortage, check with your team regarding current policies.
pRBC
- Typically transfuse if Hgb <7, sometimes <8 in cardiac patients, and in pts with active bleeding
- 1 unit (~300 ml) should raise Hgb by about 1g
Platelets
- Typically transfuse for <10k if no active bleeding, <50k if active bleeding or invasive procedure, and <100k for neurosurgical procedures or concern for active ICH
- 1 unit should raise platelets ~20k – 30k but can be variable
Acute Issues
1. Bradycardia
- Get a full set of vitals first. Go see the patient. Are they sleeping? Does the HR improve when they wake up?
- If they are symptomatic (dizzy, chest pain, syncope) or hemodynamically unstable, follow ACLS guidelines. Put patient in Trendelenburg. Call your senior and a Rapid Response.
- If stable, order atropine to the bedside and consider placing the patient on telemetry.
- Place pacer pads on the patient (can always take them off) and get stat ECG.
- If ECG shows either Type II second degree or 3rd degree AV block, consider transcutaneous pacing and possibly a transvenous pacer. Call Cardiology ASAP.
- If the patient is stable and not symptomatic, take a quick look at the chart to try and determine why this might be happening.
DDX:
- Meds: β-blockers, Calcium-channel blockers, digoxin, amiodarone, clonidine.
- Cardiac: sick sinus syndrome, inferior MI, vasovagal (usually transient), 2nd or 3rd degree AV block, junctional rhythm.
- Autonomic N.S: neurocardiogenic syncope, carotid-sinus hypersensitivity, cough/micturition/emesis/defecation induced.
- Other: idiopathic degeneration (aging), infiltrative disease in the conducting system (sarcoid, amyloid), collagen vascular disease, surgical trauma, endocarditis, hypothyroidism, hypothermia, increased intracranial pressure (Cushing's reflex), hyperkalemia, hypokalemia, OSA, normal variant (marathon runner).
If you think this is medication induced, consider holding a dose of the med if stable.
- Consider calcium or glucagon administration if you believe it to be secondary to the calcium channel or beta blocker the patient is taking.
2. Hypotension
- Ddx is quite broad but most common causes in hospital are hypovolemia (dehydration or bleeding) or infection/sepsis
- Always see what the pt's baseline BP is (cirrhotic pt may normally run 90/50).
- Ask the RN to check a manual BP before acting. If truly low, go examine pt and notify senior.
- Is patient well or ill appearing? Symptomatic (lightheaded/dizzy, AMS) or asymptomatic? Cap refill? Cool or warm extremities? Dark or bloody stools?
- Typical labs to obtain include: CMP, lactate, CBC, VBG. Labs signs of decreased end-organ perfusion/tissue hypoxia include elevated lactate, AKI, elevated LFTs
- If real, intervene as below and recheck BP frequently to assess fluid responsiveness and BP trend
3. Hypoxemia (aka low SaO2/PaO2...different from cellular hypoxia)
- Go see the patient, notify senior, and don't forget the causes of hypoxemia -> V/Q mismatch, shunt, hypoventilation, diffusion defect, low inspired FiO2
- Make sure adequate waveform on pulse ox, try replacing pulse ox if not
-
Often, if you are getting called for acute hypoxemia/desats in the hospital, it is going to be:
- Flash pulmonary edema
- Atelectasis/mucous plugging
- Aspiration pneumonitis
- Pulmonary embolism although people typically develop PE outside hospital unless not on DVT ppx, post-op patient, or onc patient
- Can also consider other etiologies: COPD/asthma exacerbation, valve failure, anaphylaxis / airway obstruction, pleural effusion
-
Most likely need CXR, VBG (better if concerned for hypercapnia)/ABG (better if concerned for hypoxemia), troponin (for the shortness of breath to r/o ACS), and EKG
- Have someone call RT, reposition pt if they cannot themselves, suction oropharynx, place on some form of O2 (nasal cannula, simple face mask, non- rebreather, venturi mask, HFNC, CPAP, BiPAP)
- CPAP for pure hypoxemia. BiPAP for hypercarbia +/- hypoxemia
- NIPPV is particularly helpful in COPD, obesity-hypoventilation, CHF/pulm edema, and post-extubation.
- It should be used in quickly reversible respiratory processes.
- Do not use if patient is altered, airway instability (like vomiting or copious secretions), or hypotensive as NIPPV decreases preload and will make worse.
- Good rule of thumb: okay to use NIPPV if RR 25-30, pH 7.25-7.35, PaCO2 45-60 Needs to be intubated if c/f airway patency, GCS <8, RR ≥35, severe dyspnea, life-threatening hypoxemia, pH <7.25 and PaCO2 >60, PaO2/FiO2 ratio <200, failure of NIPPV, persistent increased WOB
- Patients cannot stay on the floor if this is NEW CPAP/BiPAP and you are using for extended period of time. Call the ICU.
- On the floor, 6L NC is typically the limit of O2 delivery allowed long-term
Management based on probable etiology:
- Atelectasis/Mucous Plug
- If few resp secretions then can give incentive spirometer / encourage coughing / ambulate
- If abundant resp secretions then suctioning, chest PT (if able), encourage coughing, and possible intubation if unable to protect airway
- Pulmonary Edema/Fluid Overload
- Suspect in pts with hx of HF, renal failure, or receiving high rates of IVF
- CXR will show interstitial edema and you may hear crackles/see LE edema/JVD
- Stop IVF, trial IV Lasix (20-120 mg depending on renal function and naivety to Lasix)
- Nitrates can provide symptomatic relief (reduces afterload)
- Can trial BiPAP but this should be for finite time period
- Aspiration Pneumonitis/Pneumonia
- No one will ever fault you for starting empiric abx coverage (i.e. ceftriaxone unless c/f empyema or abscess. If concerned or don't know, then start zosyn +/- vancomycin if they are unstable or you know their MRSA nares screen is positive).
4. Opioid Overdose
- Suspect in any pts receiving opiates (heme/onc pts, sickle cell on PCI pump in particular) or hx of addiction - look for somnolence, pinpoint pupils, and decreased RR.
- Naloxone (Narcan) will save a life so give it if you are even thinking about it.
- Diagnosis is made by IMMEDIATE improvement in mental status / RR.
- Can start with 0.4 mg IV (or IN)
- You don't want to reverse the pain effects of opioids / precipitate withdrawal, so heme/onc pts may only need 0.1 mg as a starting dose
- Be aware you may need to redose in 30- 60 min depending on opioid.
5. Seizures
- Go see pt, ask about vital signs on your way and how long the patient has been seizing, get fingerstick glucose, place on O2/monitor, determine IV access (at least two), and have suction nearby in case they vomit.
- Make sure patient is in left lateral decubitus position
- Labs to consider include BMP, Mg, Phos, LFTs, CBC, AED levels (if appropriate), Utox, VBG/ABG, CK
- Consider lactate - but usually elevated for a few hours after seizure
Things to Think about:
- If pt has hx of epilepsy or first-time seizure as need to determine etiology (this will likely be done after the matter)
- Determine if seizure activity is suppressible ie: if R arm twitching see if you can hold it down without reciprocal movement, if they withdraw to painful stimuli
-
If the patient is stable and you have time to take a video for Neuro, it is helpful!
-
If seizing has stopped when you arrive, draw stat labs, review chart, talk to witnesses, consider CT, and AEDs as needed.
- Allow 3 min for seizure to stop spontaneously. If lasting longer, trial 2-3 mg IV lorazepam to break seizure; repeat q2-4 min until seizure stops (max at 0.1 mg/kg total, so 8 mg for 80 kg person)
- If you are needing more than 1 dose, have someone call neurology for assistance
- Be cautious about respiratory depression or hypotension with benzos
- If no IV access, ask what IM/IN options available on that floor (i.e IM midazolam 5-10 mg)
- If continues to seize and neurology isn't there yet, consider IV fosphenytoin load 20 mg/kg (can cause hypotension, works VERY fast)
- If patient required several doses of benzo to break seizure, need to load with non- benzo AED (talk to neuro but consider keppra, fosphenytoin, valproate).
Less Acute but Common Complaints
1. Anxiety
- Assess why the patient is anxious.
- Good first line med is Vistaril – typical starting dose is 25 mg for anxiety but can give lower dose if c/f sedation (don't give to elderly).
- For select pts, can consider lorazepam (Ativan) – typically would start at low doses such as 0.25 – 0.5 mg PO. Benzos can worsen delirium in pts that are already agitated and should be avoided in the elderly.
- For pt with delirium and anxiety, can trial low dose PO/IV Haldol if QTc permits (<500).
2. Acute Pain
- First assess vitals and mental status. If BP already low and/or altered, avoid opiates if able. You can utilize nursing input to assess mental status.
- Is it somatic pain, visceral pain, or neuropathic pain?
- Consider renal function and LFTs when choosing med.
- Tylenol is good starting med (limit 4 g per day in most patients and 2 g per day in pts with cirrhosis).
- Can give NSAIDs to select group of pts (contraindicated in renal disease, heart disease, cirrhosis, thrombocytopenia, etc).
- Heat and topicals such as capsaicin cream or lidocaine patches are great for localized pain.
- Neuropathic pain: can consider agents like gabapentin, pregabalin, and/or amitriptyline
- Opioids are typically the next step IF somatic pain (watch for resp depression – see section on opioid overdose in Hypoxemia section)
- Typical rule of thumb is use oral form if able to take PO.
- Oxycodone: 2.5-5mg q4-6h for those who are relatively opioid naïve. Comes in PO or liquid.
- Morphine: IV/PO/liquid. Avoid in renal dysfunction. Starting doses typically 10-15 mg PO or 2-4 mg IV for naïve patients
- Hydromorphone (Dilaudid): IV/PO. 10x more potent than morphine. Typical starting dose is 2-4 mg tablets (different dosage for solution) or 0.2-0.5 mg IV for naïve patients
3. Headache
- Assess patient's clinical status and severity of headache
- If severe, eval patient and perform neuro exam / consider CT Head to r/o brain bleed.
- What do they take at home for headaches?
- Safest medication in hospital is Tylenol (can give up to 2 g in liver pts)
- 2g IV magnesium is also great for headaches (can give 400mg PO too)
- Can give NSAIDs to pts w/o contraindications
- Consider headache cocktail (ex: 975 mg of acetaminophen, IV 5 mg Compazine or PO 10mg, and/or PO 25 mg Benadryl)
- AVOID NARCOTICS
4. Insomnia
- The hospital is not a restful place for even the greatest of sleepers
- Be sure to ask RN to make sure TV and lights are off in the room and noises/distractions minimized
- Ask what patient takes at home for sleep / check home meds
- If pt does not take anything, would trial ramelteon 8 mg or melatonin.
- Second line option includes trazodone
5. Nausea
- First line: ondansetron (Zofran) – usual dose is 4-8 mg IV/PO/ODT
- Second line: consider prochlorperazine (Compazine), lorazepam, or Benadryl
- Compazine: oral 10 mg tablets q6h prn (or IV 5-10 mg)
- Other options include low dose Zyprexa (olanzapine)/Haldol, metoclopramide, or promethazine
- Ondansetron, Haldol, and metoclopramide can prolong QTc. You do not necessarily have to check it on everyone but get EKG on those requiring high / frequent doses or are on other meds that prolong QTc
6. Pruritus
- Good go-to med is Atarax 10 mg TID PRN as it is typically not as sedating as Benadryl
- Sarna or Lac-Hydrin lotion are good topical options
- Can also consider PO Benadryl 12.5 – 25 mg but typically avoid in pts with AMS and older pts
- Reserve use of IV Benadryl for pts who cannot tolerate PO or those who have an allergic rxn as it can cause a euphoric effect similar to opiates.
7. Constipation
- Especially since almost everyone is on narcotics for pain control.
- Colace 100 mg PO BID and Senna® 2 tabs PO qHS are essential. Glycolax is also a good option.
- Be sure to add a HOLD order for loose stools as well.
- The problem arises when Colace, Senna, or Glycolax are not doing the trick; this is where PRN bowel care will help you and the nursing staff out. You can dose with milk of magnesia 30 cc PO PRN constipation. If that does not work, I move on to Dulcolax 10 mg PO/ PR (per rectum) daily PRN no bowel movement. The last resort, to my mind, is lactulose 30 mL PO q4h until bowel movement, or a "pink lady" enema once; these will usually get things moving.
Disclaimer
Always verify with your superiors before taking action based on this guide. The information is intended to help, but not to dictate your course of work. Always use critical judgment and your clinical knowledge skills. This guide will be constantly revised and updated according to evidence-based medicine.
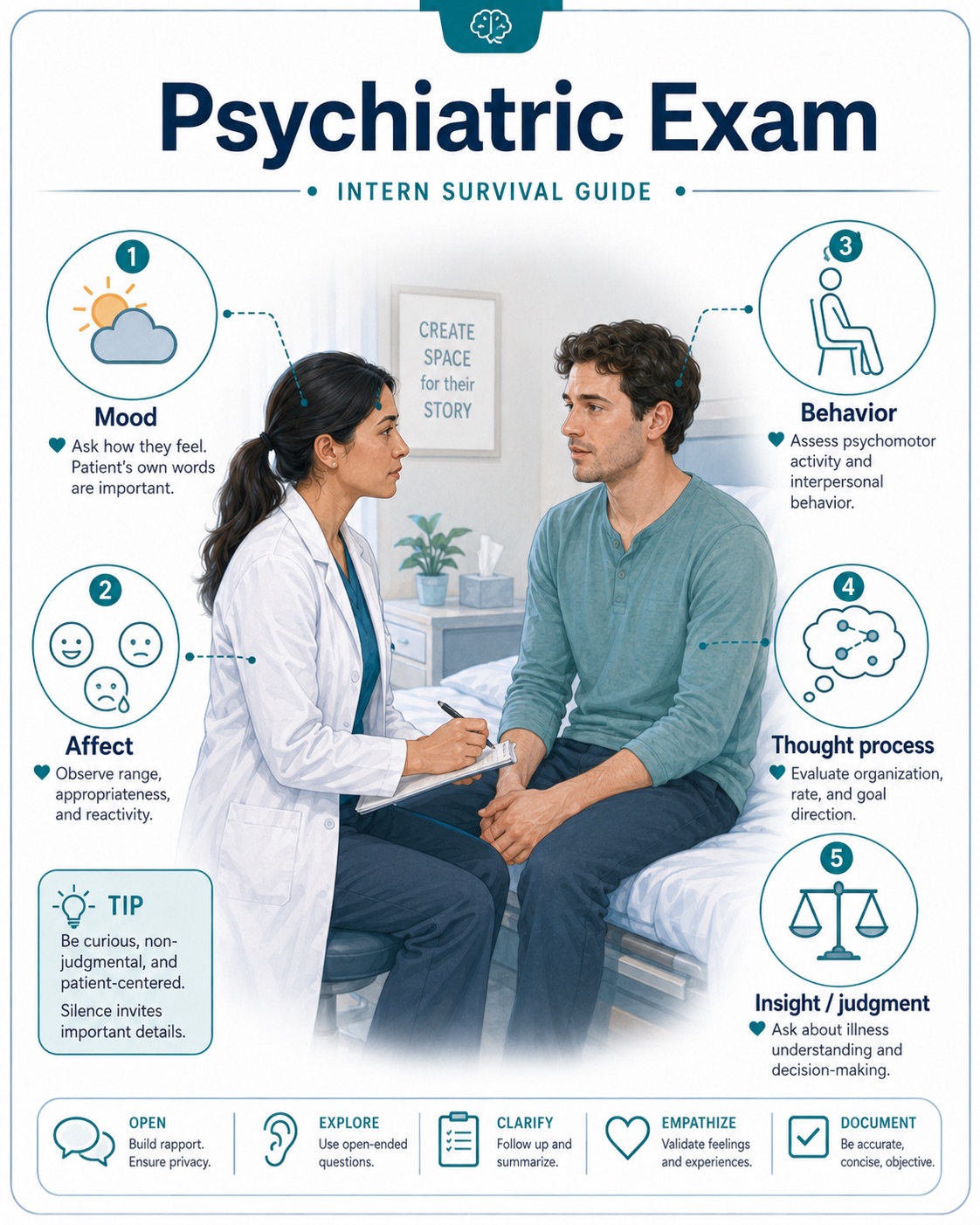
Physical Exam for New Interns
A focused, reliable physical exam is one of the most important skills for interns. It helps you identify clinical changes early, communicate clearly with attendings and consultants, and document findings that support your assessment and plan. The goal is not to perform a full head-to-toe exam on every patient every day, but to perform a thoughtful exam based on the patient's chief complaint, active problems, and overnight events.
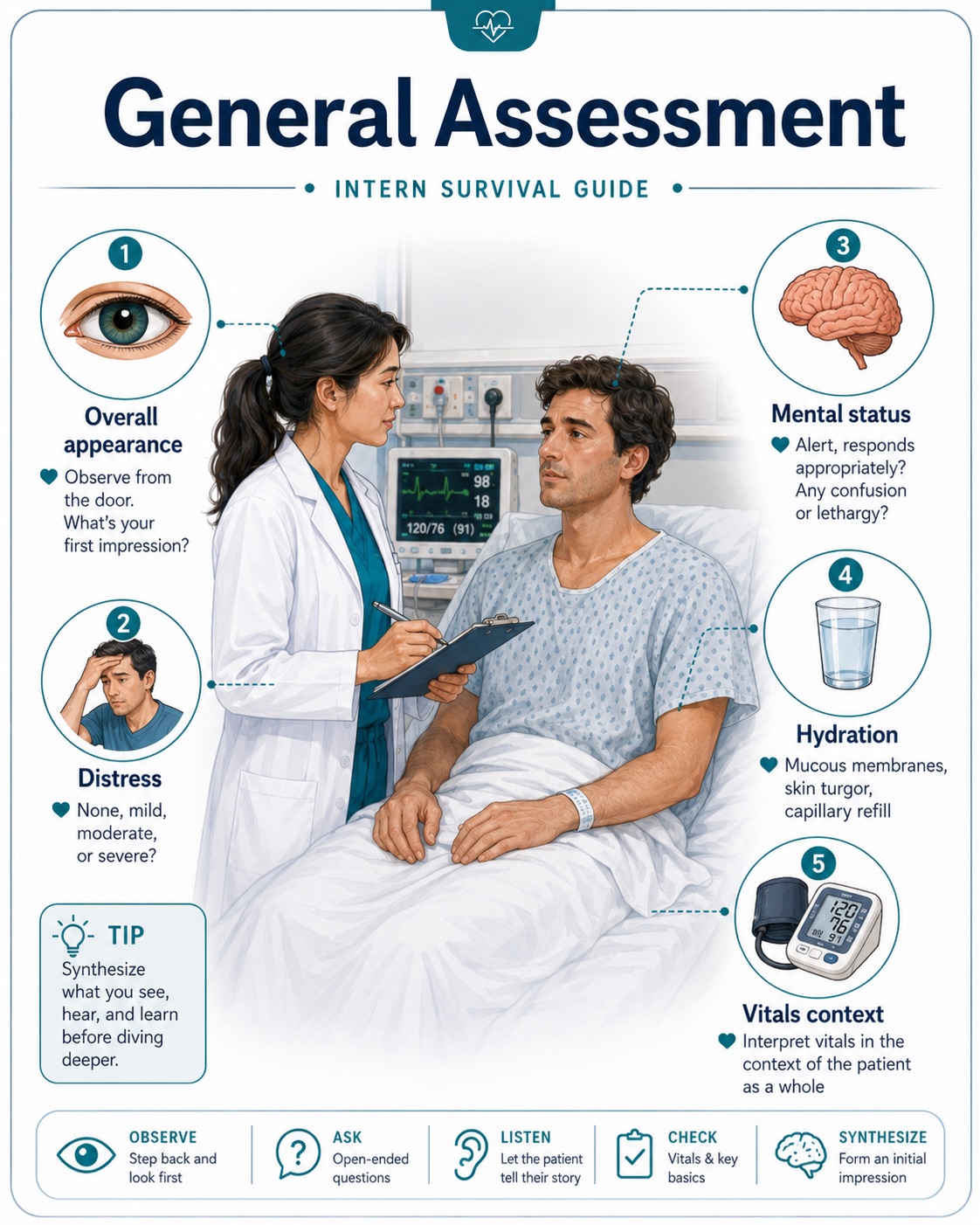
General Approach
Before entering the room, briefly review the patient's diagnosis, vitals, overnight events, labs, imaging, oxygen requirement, and current treatment plan. This helps you know what findings to look for.
Always start with the patient's overall appearance. Ask yourself: Does the patient look comfortable or toxic? Are they in distress? Are they awake, confused, lethargic, or agitated? Are they breathing comfortably? Are they able to speak in full sentences?
The One Question Every Daily Exam Should Answer
"Is this patient better, worse, or unchanged compared with yesterday?"
Basic Daily Physical Exam Template
General: Alert and oriented, no acute distress, appears comfortable/uncomfortable, ill-appearing, toxic-appearing, or lethargic.
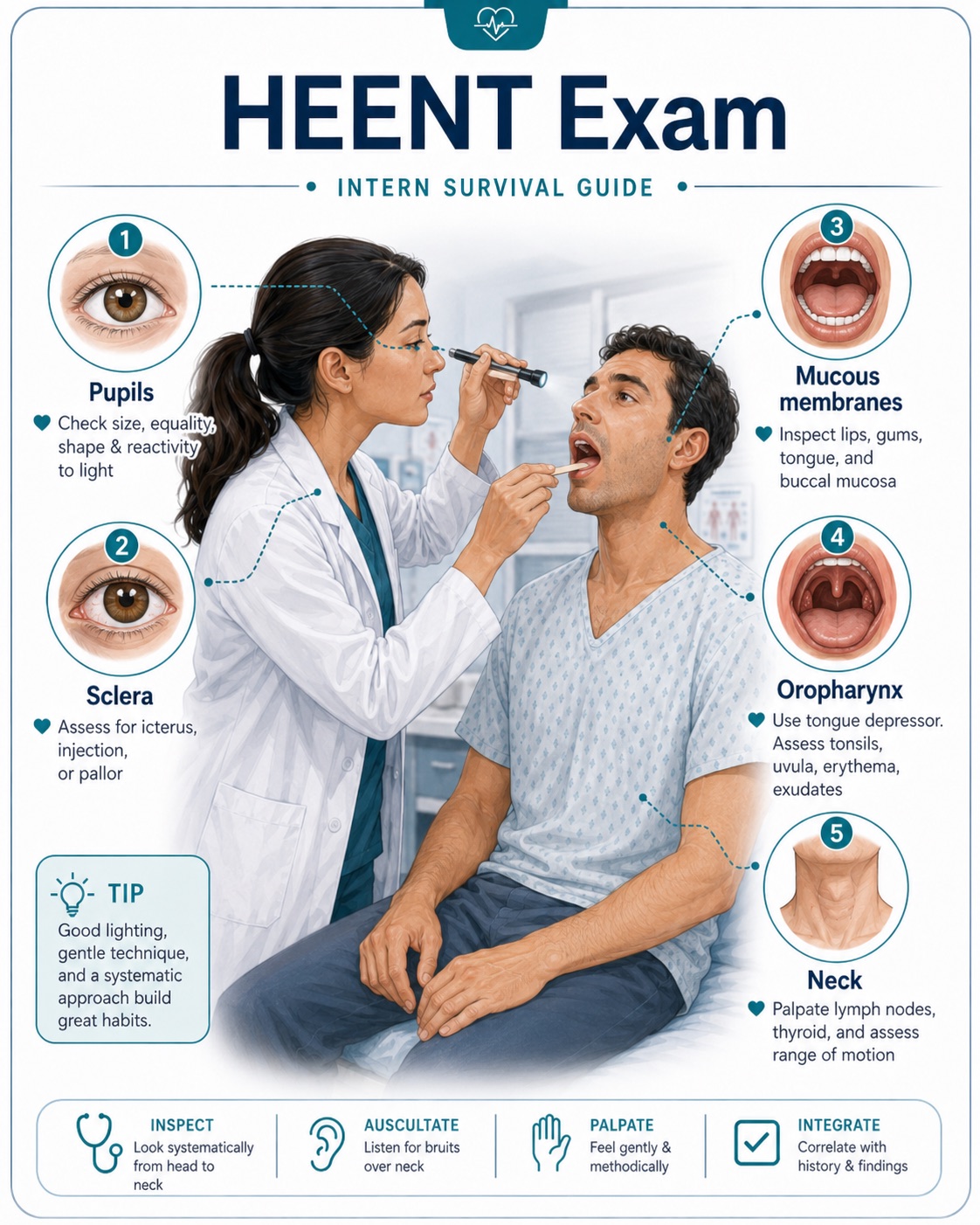
HEENT: Normocephalic, atraumatic. Pupils equal and reactive if relevant. Mucous membranes moist or dry. No scleral icterus.
Cardiovascular: Regular rate and rhythm. No murmurs, rubs, or gallops. Peripheral pulses intact. Assess for JVD and lower extremity edema when evaluating volume status or heart failure.

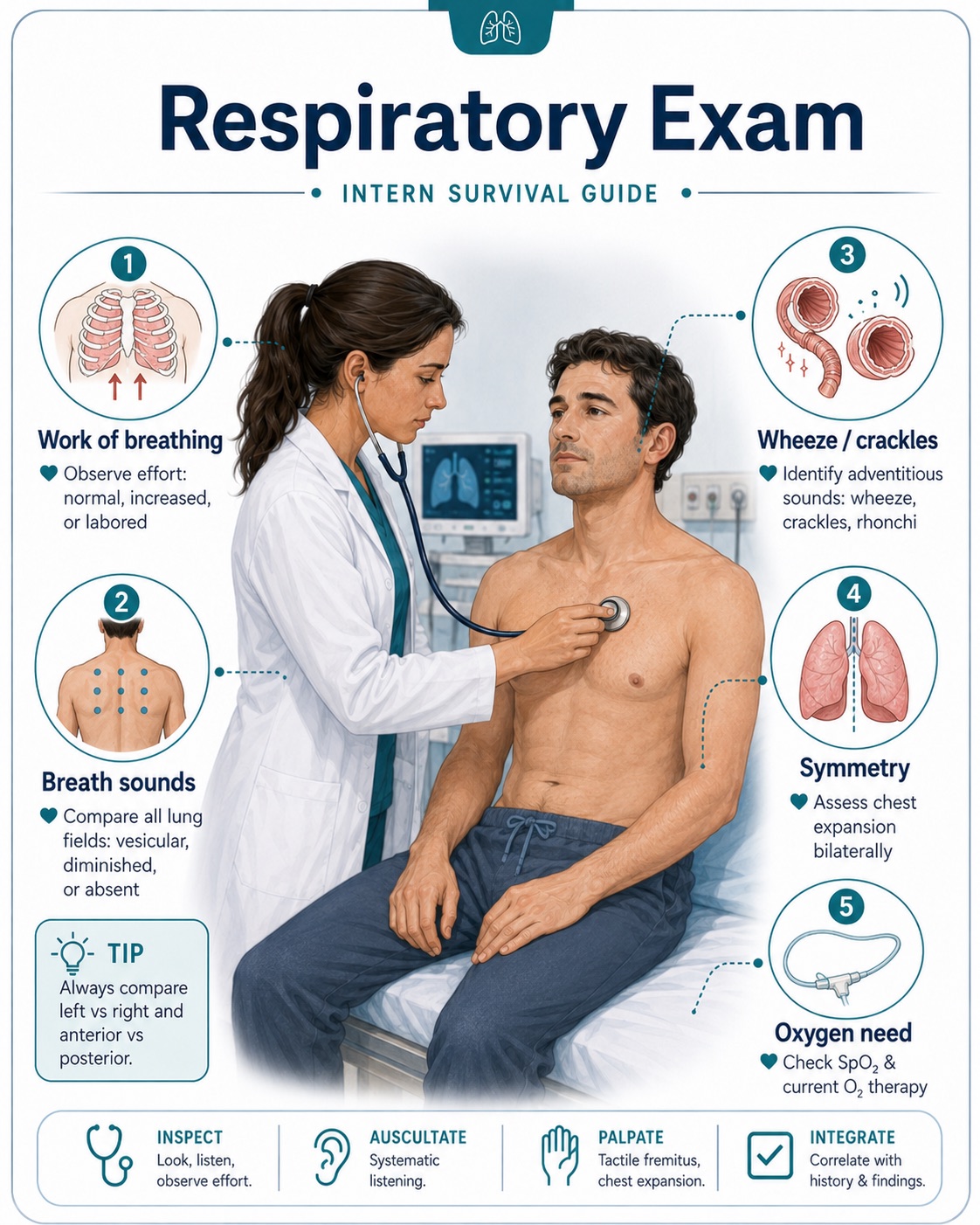
Respiratory: Normal work of breathing. Clear to auscultation bilaterally, or note wheezing, crackles, rhonchi, diminished breath sounds, accessory muscle use, or oxygen requirement.
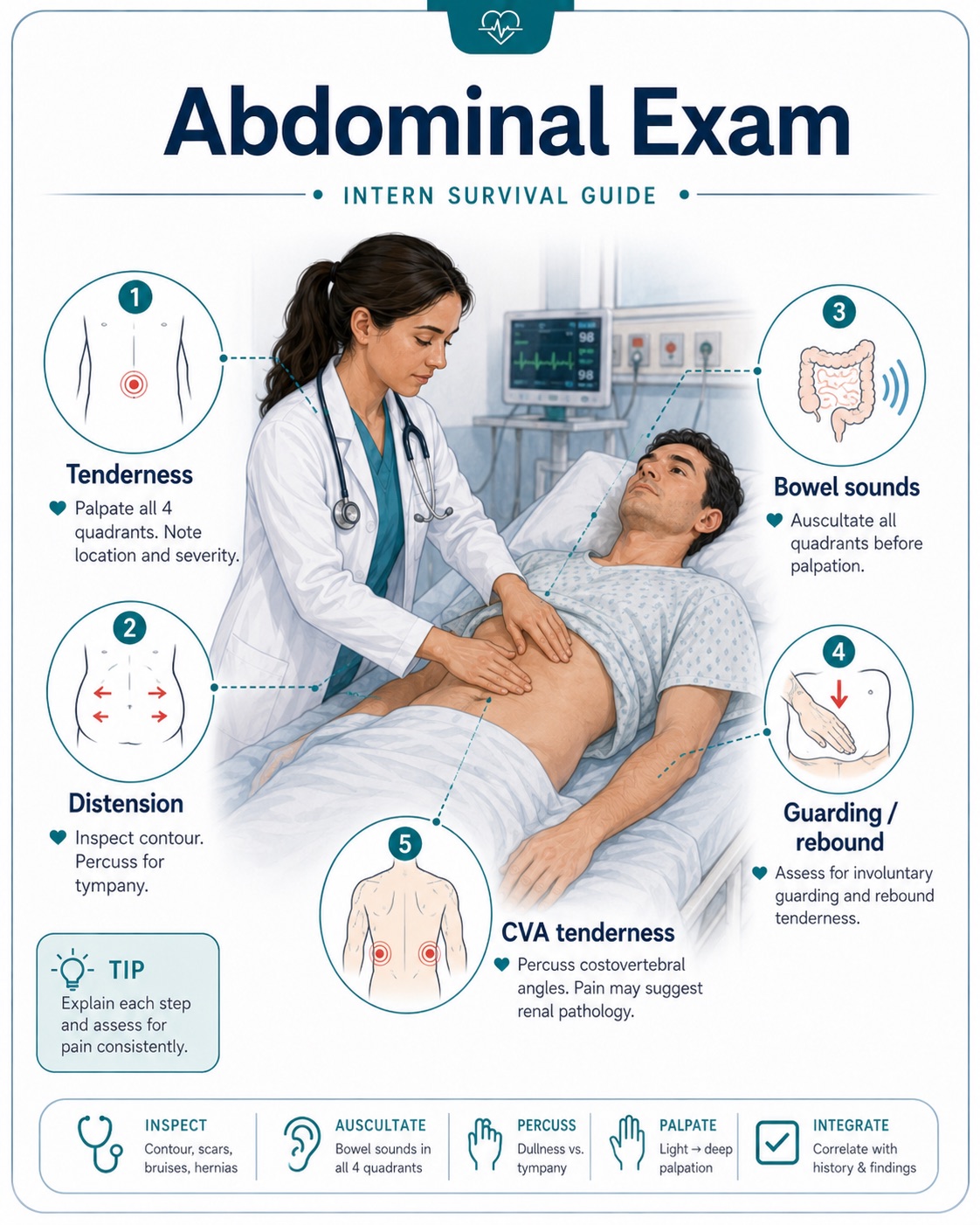
Abdomen: Soft, non-distended, non-tender. Bowel sounds present. Note guarding, rebound, rigidity, suprapubic tenderness, or CVA tenderness when relevant.
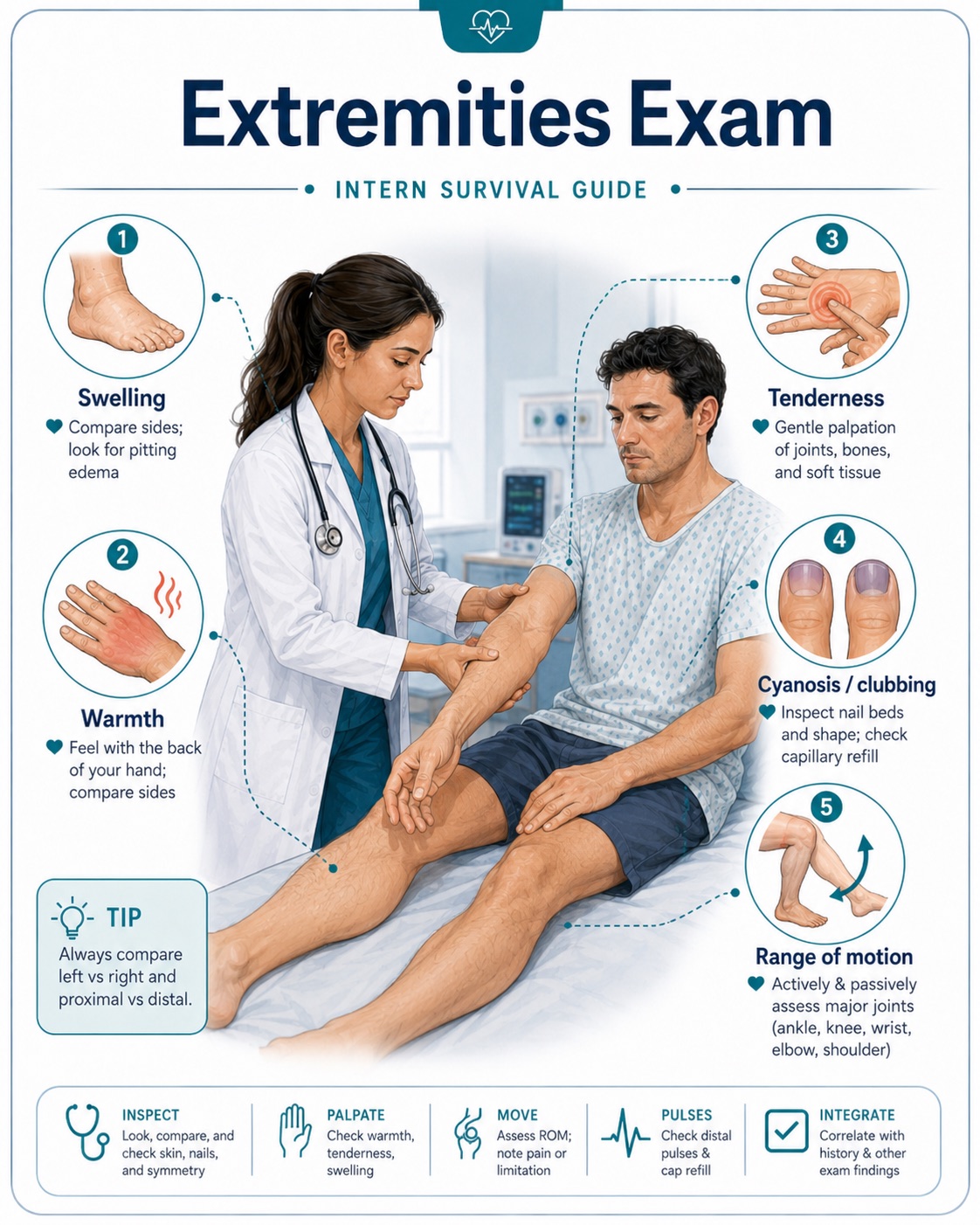
Extremities: No edema, cyanosis, or clubbing. Assess tenderness, erythema, warmth, swelling, range of motion, and pulses when indicated.
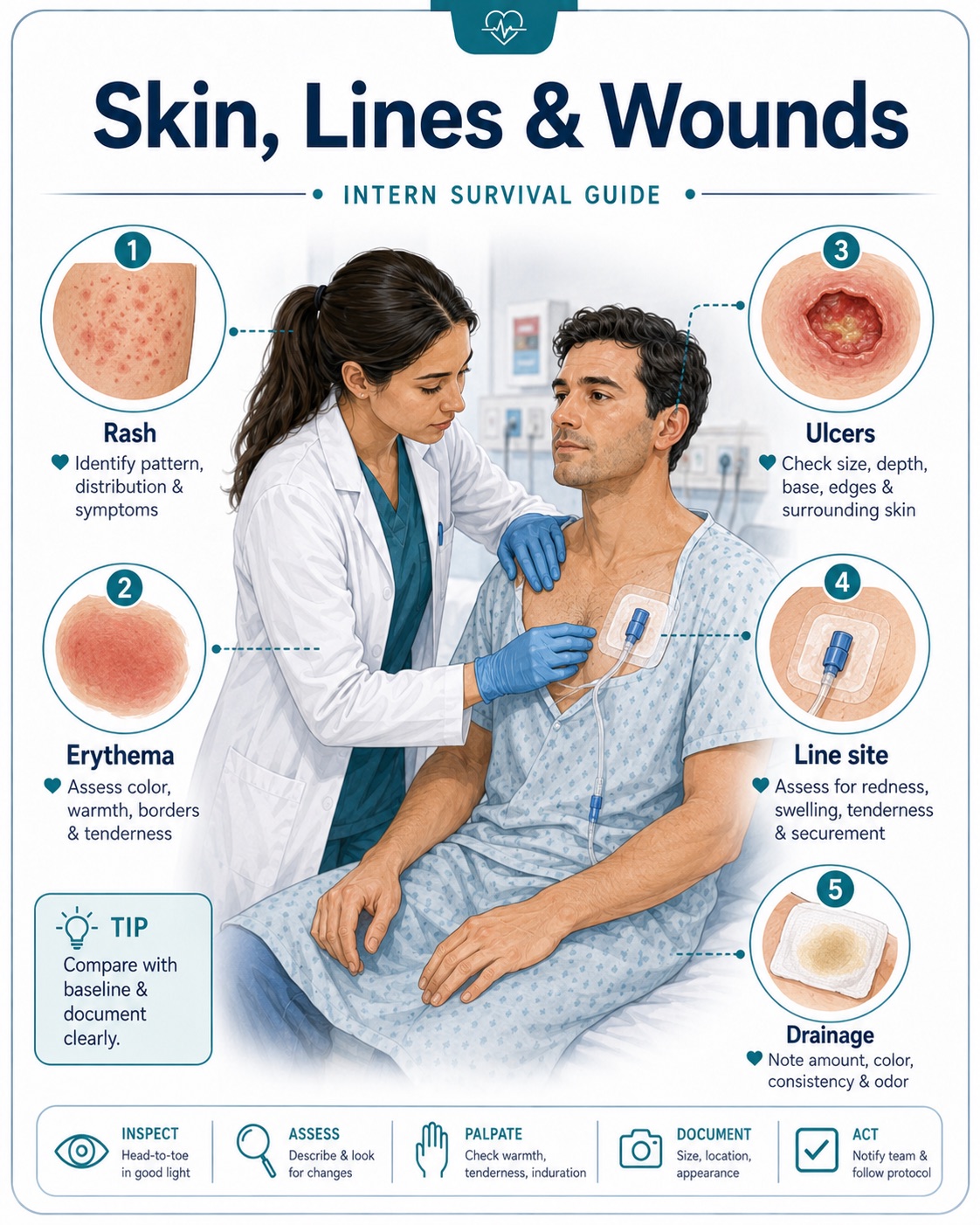
Skin: Warm and dry. No rash, wounds, ulcers, cellulitis, bruising, or pressure injuries. Examine lines, drains, and surgical sites when present.
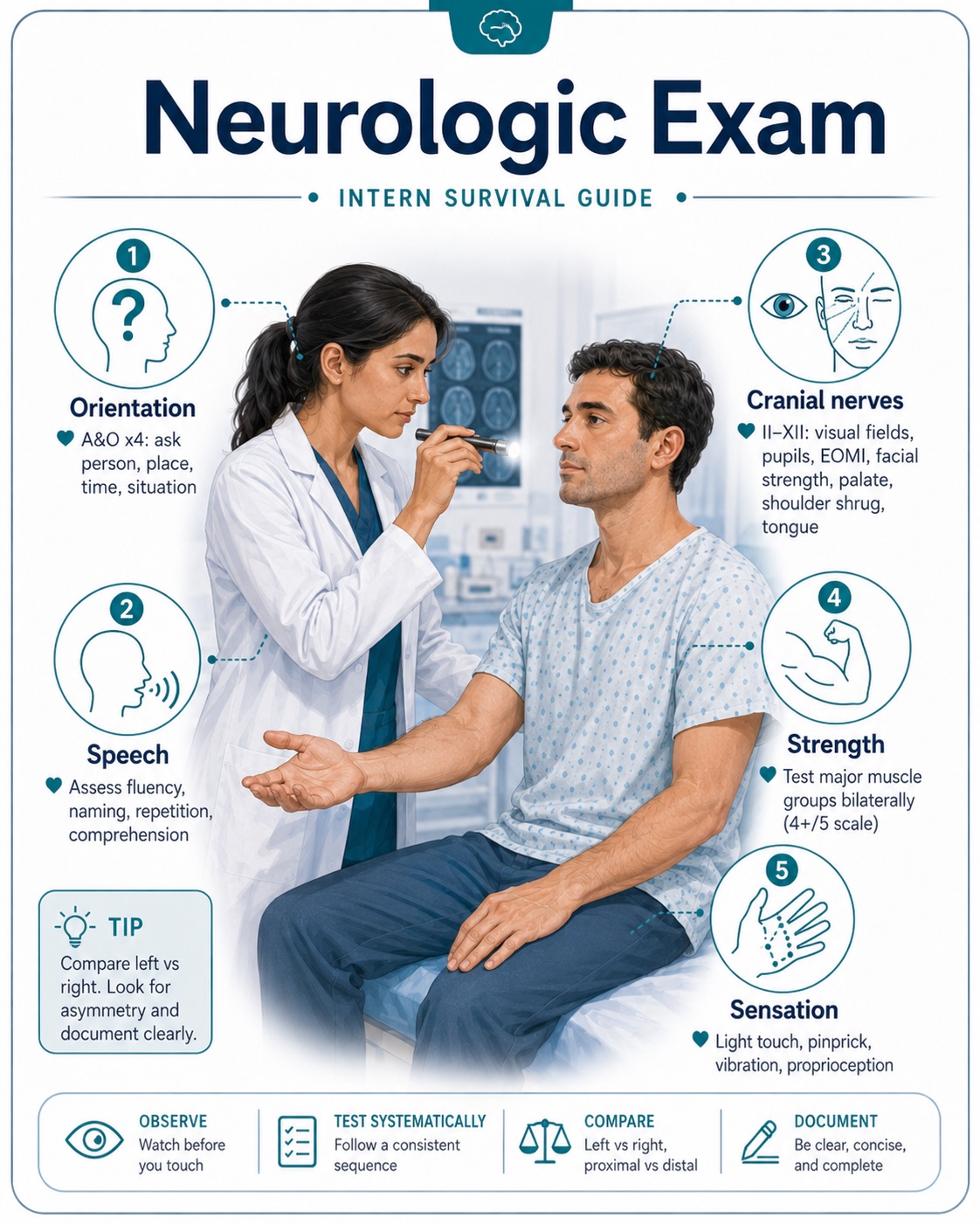
Neurologic: Awake and oriented. No focal deficits. Strength and sensation grossly intact. Cranial nerves, pronator drift, speech, gait, or cerebellar testing if stroke, weakness, dizziness, or altered mental status is a concern.
Psychiatric: Appropriate mood and affect. Cooperative, anxious, agitated, confused, or withdrawn when clinically relevant.
High-Yield Exam Findings by System
Cardiovascular
For chest pain, heart failure, syncope, arrhythmias, or shock, focus on:
- Heart rate and rhythm
- Murmurs, especially new systolic murmur
- JVD
- Peripheral edema
- Peripheral pulses
- Capillary refill and extremity temperature
- Signs of volume overload or poor perfusion
Useful documentation examples:
- "Regular rate and rhythm, no murmurs, no JVD, no bilateral lower extremity edema."
- "Irregularly irregular rhythm, tachycardic, 2+ bilateral lower extremity edema, mild JVD."
- "Extremities cool to touch with delayed capillary refill, concerning for poor perfusion."
Respiratory
For shortness of breath, pneumonia, COPD/asthma, CHF, hypoxia, or PE concern, assess:
- Work of breathing
- Ability to speak in full sentences
- Oxygen requirement
- Crackles, wheezing, rhonchi, or diminished breath sounds
- Accessory muscle use
- Symmetry of breath sounds
Useful documentation examples:
- "Normal work of breathing on room air, lungs clear to auscultation bilaterally."
- "Diffuse bilateral expiratory wheezing with prolonged expiratory phase."
- "Bibasilar crackles with decreased breath sounds at the right lung base."
- "Increased work of breathing with accessory muscle use, requiring 4 L nasal cannula."
Abdomen
For abdominal pain, GI bleed, pancreatitis, obstruction, urinary symptoms, or sepsis, assess:
- Tenderness location
- Distension
- Guarding, rebound, or rigidity
- Bowel sounds
- CVA tenderness
- Suprapubic tenderness
- Surgical scars, drains, PEG tube, ostomy, or wounds
Useful documentation examples:
- "Abdomen soft, non-distended, mild epigastric tenderness, no rebound or guarding."
- "Diffuse abdominal tenderness with voluntary guarding, no rigidity."
- "Left CVA tenderness present."
- "Suprapubic tenderness present, no rebound or guarding."
Neurologic
For altered mental status, stroke symptoms, falls, dizziness, weakness, or seizures, assess:
- Alertness and orientation
- Speech
- Pupils
- Facial symmetry
- Strength in all extremities
- Sensation
- Pronator drift
- Coordination if relevant
- Gait if safe
Useful documentation examples:
- "Alert and oriented x3, speech clear, no facial droop, strength 5/5 in all extremities, sensation intact."
- "Confused but awake, oriented to self only, follows simple commands, no obvious focal motor deficit."
- "Right-sided facial droop with 4/5 strength in right upper and lower extremities."
Musculoskeletal
The musculoskeletal exam is especially important for patients presenting with falls, joint pain, back pain, weakness, trauma, inability to ambulate, cellulitis vs. septic arthritis, gout, or functional decline. Assess:
- Pain location and severity
- Joint swelling, erythema, warmth, or deformity
- Range of motion, both active and passive if tolerated
- Tenderness to palpation
- Strength in major muscle groups
- Gait and ability to bear weight, if safe
- Spine tenderness, especially after falls or trauma
- Signs of inflammatory arthritis, gout, septic arthritis, or fracture
Useful documentation examples:
- "Normal range of motion in bilateral upper and lower extremities. No joint swelling, erythema, warmth, or deformity."
- "Right knee with mild swelling and tenderness to palpation, no erythema or warmth. Range of motion limited due to pain."
- "Left hip tender to palpation with limited range of motion due to pain. Patient unable to bear weight."
- "Midline lumbar spine tenderness present. No obvious step-off or deformity."
- "Bilateral knees with chronic osteoarthritic changes, no acute swelling, erythema, or warmth."
Don't Miss Septic Arthritis
For suspected septic arthritis, carefully document whether the joint is warm, swollen, and erythematous, and whether passive range of motion is painful. A hot, swollen joint with severe pain on passive range of motion should prompt urgent evaluation.
Skin, Lines, and Wounds
Do not forget to examine lines, wounds, and devices. These are common sources of infection and complications. Check:
- Peripheral IV sites
- PICC lines and central lines
- Foley catheter
- Surgical incisions
- Pressure injuries
- Diabetic foot wounds
- Drain sites
- PEG/trach sites
Useful documentation examples:
- "PICC line site clean, dry, and intact without erythema or drainage."
- "Sacral pressure injury noted with surrounding erythema, no purulent drainage."
- "Right foot ulcer with surrounding warmth and erythema, no crepitus."
Exam Tips for Interns
- Document only what you actually examined. Avoid copying forward an exam that was not performed.
- Compare with prior exams. If crackles, edema, confusion, weakness, or abdominal tenderness are improving or worsening, mention the trend.
- Use specific language. Instead of "normal neuro exam," write the key findings: orientation, speech, strength, facial symmetry, and focal deficits.
- Always reassess patients with clinical changes. New fever, hypotension, tachycardia, hypoxia, chest pain, altered mental status, abdominal pain, or a fall should prompt a bedside exam.
- For unstable patients, start with ABCs: airway, breathing, circulation. Check mental status, vitals, oxygen requirement, work of breathing, pulses, perfusion, and signs of shock.
Focused Exam Examples
Chest Pain
General appearance, vitals, cardiac exam, lung exam, chest wall tenderness, pulses, lower extremity edema, signs of DVT if PE is considered.
"Patient comfortable, no acute distress. Regular rate and rhythm, no murmurs. Lungs clear bilaterally. No chest wall tenderness. No lower extremity edema or calf tenderness."
Shortness of Breath
Work of breathing, oxygen requirement, lung sounds, JVD, edema, heart rhythm, mental status.
"Mild increased work of breathing on 3 L nasal cannula. Bibasilar crackles present. Mild JVD and 1+ bilateral lower extremity edema."
Abdominal Pain
Pain location, distension, bowel sounds, rebound, guarding, rigidity, CVA tenderness, suprapubic tenderness.
"Abdomen soft, mildly distended, tender to palpation in right lower quadrant, no rebound or guarding."
Altered Mental Status
Orientation, attention, speech, pupils, facial droop, strength, sensation, signs of infection, respiratory status, medication/sedation effects.
"Awake but confused, oriented to self only. Speech fluent. No facial droop. Moves all extremities spontaneously. No focal neurologic deficit appreciated."
Fall
Head trauma, neck/back pain, focal neuro deficits, extremity pain, range of motion, gait if safe, anticoagulation status.
"Patient evaluated after fall. No visible head trauma. No cervical spine tenderness. Alert and oriented x3. No focal neurologic deficits. Full range of motion of bilateral upper and lower extremities without deformity."
Volume Status
Volume assessment is very common but can be difficult. Look for mucous membranes, skin turgor, JVD, lung crackles, peripheral edema, daily weight, intake/output, blood pressure and heart rate trends, creatinine/BUN trend, and response to fluids or diuretics.
"Exam concerning for volume overload with bibasilar crackles, elevated JVD, and 2+ bilateral lower extremity edema."
"Appears volume depleted with dry mucous membranes, tachycardia, and poor oral intake."
Sepsis Concern
General appearance, mental status, perfusion, capillary refill, skin temperature, lung exam, abdominal exam, CVA tenderness, lines/wounds.
"Ill-appearing and febrile. Tachycardic. Extremities warm with intact pulses. Lungs with right basilar crackles. Abdomen soft and non-tender. No CVA tenderness. PICC site without erythema or drainage."
Final Reminder
A strong physical exam does not need to be long. It needs to be accurate, focused, and clinically useful. When in doubt, go to bedside, examine the patient yourself, and document what changed.
 Contributed by Mafaz Mansoor, MD
Contributed by Mafaz Mansoor, MD
Common Problems in Adult Medicine
Cardiology
- Keep K+ above 4 and Magnesium above 2 (don't replace for patients with ESRD or ARF unless you talk to someone first).
- Always compare ECGs to old.
- PO to IV furosemide is 2:1 (i.e. 40 mg of PO furosemide is 20 mg IV)
- PO hydralazine to IV hydralazine is 4:1.
- Toprol XL to metoprolol is 1.4 mg to 1 mg. Hold all beta-blockers for >12 hours in patients who are getting a stress test.
- Dry lungs are happy lungs. Diuresis will be used often.
- Beers Criteria lists many medications that should be avoided in "older adults."
Chest Pain
Relevant questions: Based on possible cause, ruling out scary stuff.
- Acute Coronary Syndrome (ACS): typically pressure type of pain, associated with shortness of breath, nausea, vomiting, diaphoresis, radiation. Assess for risk factors including history of prior MI, prior stenting procedures, DM, HTN, tobacco use, FHX, hyperlipidemia. MI can present atypically in women and diabetics.
- Aortic dissection: "tearing" pain that usually radiates to the back. Associated with HTN, smoking.
- Pneumothorax: Associated with COPD, trauma, central lines. Decreased breath sounds, hyperresonance. Deviation of the trachea away from the side of the PTX, hypoxia.
- PE: dyspnea, tachycardia, tachypnea, pleuritic chest pain, hypoxia, A-a gradient, possible hemoptysis.
Focused Exam
- Vital signs and pulse ox
- JVD, Hepatojugular reflux
- Cardiac exam
- Lung exam
Data
- EKG
- Electrolytes to assess bicarb, K, BUN, Cr and glucose
- CBC
- Troponin
- CTPE if concern for PE
| Type | Troponins | ECG changes |
|---|---|---|
| STEMI | Positive | ST elevations or new LBBB |
| NSTEMI | Positive | May have ST depressions, T wave inversions, or ST elevations that don't meet criteria for STEMI |
| Unstable angina | Negative | +/- May have ST depressions, T wave inversions, or ST elevations that don't meet criteria for STEMI |
Treatment
- Telemetry
- Exact treatment depends on etiology - obtain EKG and discuss with senior
- Probable Cardiology consult.
Daily F/U
- Vitals and 02 sat
- Adequacy of symptoms control
Atrial Fibrillation
Relevant questions
- Symptoms: palpitations, syncope, chest pain
- Medication adherence issues ?
- Ever been told about atrial fibrillation before?
- On anticoagulation? Which medication? Compliant?
Focused Exam
- Cardiac exam
- JVD, carotid bruits
- Brief neurologic exam
Data
- EKG
- Electrolytes to assess bicarb, K, BUN, Cr and glucose
- TSH reflex
- CBC
- Troponin
Treatment
- If hemodynamically unstable: cardioversion (synchronized, start 200 J)
-
If stable, control rate
- Tip: be careful when using β-blockers and Calcium channel blockers together, as the combination may cause excessive AV nodal blockade.
-
β-blockers: don't give if actively wheezing or if in decompensated heart failure.
i. Metoprolol PO if rate is relatively slow and patient is stable
ii. Metoprolol 5 mg IV X 3
iii. Esmolol gtt- good to consider in ICU patients
-
Calcium channel blockers: Contraindicated with VT, 2nd /3rd degree heart block without pacer, severe hypotension, cardiogenic shock, bypass tracts, EF < 40%
i. Diltiazem: bolus administration (0.25 mg/kg up to 20 mg) and if that does not work, then gtt
-
Digoxin: caution in renal failure. Less hypotension. Controls rate at rest, but not with exercise. Slower onset. Remember to check levels.
- Amiodarone: long term side effects. Consider in unstable patients or patients with CHF who need rate and rhythm control, do not order without senior as patients who are not anticoagulated can revert to sinus rhythm and throw a clot
-
Anticoagulation
- Do they need it? Calculate Chads2Vasc
- Discuss with team based on comorbidities and likelihood of adherence - DOAC vs Warfarin (UpToDate guidance here)
Daily F/U
- Telemetry monitor
- Vitals - HR and BPs especially
- Ability to hold conversation, move around in room and attend to personal needs
- Adequacy of rate control - goal <110 bpm
- Patient/family understanding of progress and plan, and expectation for discharge
CHF Exacerbation
Relevant questions
-
Symptoms
- Quantify exercise tolerance and compare to baseline
- Length of symptoms
- Change in shortness of breath
- Change in leg swelling or weight
-
Any dietary changes?
- Has there been a need to use more diuretics?
- Inability to get or take medications
- Dry weight? (weight when adequately diuresed)
- Setting-from home or nursing home
Focused Exam
- Vital signs and pulse ox
- Able to speak in complete sentences?
- Respiratory rate and work of breathing
- Leg edema
- JVD and HJR
- Cardiac - murmur, gallop?
- Lungs-Breath sounds, crackles to where?
Data
- CXR on admission and with clinical change
- EKG
- Electrolytes to assess bicarb, K, BUN, Cr and glucose
- BNP
- Consider troponin if pain
- CBC
Treatment
- 02 to oxygen saturation > 88%
- Volume guided diuresis: diuresis to dry body weight or renal stress
- Can use: Lasix, bumex, torsemide.
- Lasix usually first line unless patient does not respond.
- If patient is not Lasix-naive, will need to double their home dose and see how much they put out
- Daily weights and strict I/Os
- DVT prophylaxis (heparin for Cr clearance < 30)
Daily F/U
- Vitals and 02 sat
- Ability to hold conversation, move around in room and attend to personal needs
- Weight, net negative volume
- Edema, lung exam, JVD
- Patient understanding of progress and plan, and expectation for discharge
- Follow up with family if needed
Pulmonology
Pneumonia
Relevant questions
-
Symptoms
- Quantify exercise tolerance and compare to baseline
- Length of symptoms
- Cough? With sputum?
-
Any exposures?
- Sick contacts
- Environmental
- Tobacco use, prior or current
-
Prior pneumonias?
- Setting: from home or nursing home, recent hospitalizations
Focused Exam
- Vital signs and pulse ox
- Able to speak in complete sentences?
- Respiratory rate and work of breathing
- Accessory muscle use
- Lungs-Breath sounds, Air Exchange
Data
- CXR on admission and with clinical change
- EKG
- Electrolytes to assess bicarb, K, BUN, Cr and glucose
- CBC
- ABG/VBG if concern for acidosis or failure to compensate (helpful to know baseline pCO2)
- RPP
Treatment
- 02 to oxygen saturation > 88%
- Antibiotics - options include respiratory fluoroquinolone (but not if prolonged QTc), macrolide, ceftriaxone.
- Respiratory care protocol - incentive spirometer.
- DVT prophylaxis (heparin for Cr clearance < 30)
Daily F/U
- Vitals and 02 sat
- Ability to hold conversation, move around in room and attend to personal needs
- Adequacy of symptoms control
- Day of hospitalization and course of antibiotics
- Need for further reimaging
- Patient understanding of progress and plan, and expectation for discharge
- Follow up with family if needed
COPD Exacerbation
Relevant questions
-
Symptoms
- Quantify exercise tolerance and compare to baseline
- Length of symptoms
- Change in sputum
- Change in cough
- Increase in oxygen requirement (how many liters do they use at home)
-
Any exposures?
- Sick contacts
- Environmental
-
Has there been a need to use more medication?
- Inability to get or take medications
- Setting-from home or nursing home
Focused Exam
- Vital signs and pulse ox
- Able to speak in complete sentences?
- Respiratory rate and work of breathing
- Accessory muscle use
- Paradoxical breathing
- Lungs-Breath sounds, Air Exchange
Data
- CXR on admission and with clinical change
- EKG
- Electrolytes to assess bicarb, K, BUN, Cr and glucose
- CBC
- ABG/VBG if concern for acidosis or failure to compensate (helpful to know baseline pCO2)
- RPP
Treatment
- 02 to oxygen saturation > 88%
- Bronchodilators via MDI with spacer during COVID-19 outbreak (albuterol and ipratropium)
-
Steroids
- 40mg daily for 5 days. IV Solu-Medrol initially in severe presentation.
-
Antibiotics-azithromycin 500 mg for 3 days
- DVT prophylaxis (heparin for Cr clearance < 30)
Daily F/U
- Vitals and 02 sat
- Ability to hold conversation, move around in room and attend to personal needs
- Adequacy of symptoms control
- Day of hospitalization and course of antibiotics
- Need for further reimaging
- Patient understanding of progress and plan, and expectation for discharge
- Follow up with family if needed
Gastroenterology
GI Bleed
Relevant questions
-
Symptoms
- When did it start
- Number of episodes
- Associated lightheadedness, palpitations, syncope, pain?
- What does the emesis (or BM) look like? Bright red blood or dark blood?
- For BM - black, tarry = melena
- Medication use - especially NSAIDs, anticoagulants
- Alcohol use? How much (get specific)?
- Prior bleeding history?
- Liver disease? Known GI disease?
Focused Exam
- Vital signs
- Orthostatic blood pressure: + indicates ~20% volume loss
- Abd exam - tenderness? Hepatomegaly?
- Skin exam - jaundice, spider angiomata, bruising
- Consider rectal exam
Data
- Type & screen
- Electrolytes to assess bicarb, K, BUN, Cr and glucose (
BUN >> Cr suggests upper GI bleed) - CBC - discuss interval of repeat with team
- Coags - PT/INR, PTT
- EKG
Treatment
- 2 large bore IVs
- NPO and GI consult
- Transfuse for Hgb <7
- IV PPI - Pantoprazole 40 mg IV BID
- HOLD DVT prophylaxis
Daily F/U
- Vitals
- Further episodes of bleeding
- CBC stability
- GI recommendations, need for further testing
- Patient understanding of progress and plan, and expectation for discharge
- Follow up with family if needed
Transaminitis, Hepatic Encephalopathy
Relevant questions
-
Symptoms
- Abdominal pain
- Last known normal if encephalopathic
- Alcohol consumption? How much, when last (to figure out risk of withdrawal seizure)
-
Any medications? Using too much tylenol?
- Who is their GI specialist?
Focused Exam
- Vital signs
- Orientation/mental status
- Neuro: Look specifically for asterixis, ataxia, slurred speech
- Abdominal exam - hepatomegaly, abdominal pain, ascites (is there enough to tap - figure that out BEFORE antibiotics)
- Skin exam - jaundice, spider nevi
Data
- Electrolytes to assess bicarb, K, BUN, Cr and glucose
- LFTs
- PT/INR
- Consider: acute hepatitis panel, iron studies, serology for CMV and EBV
- RUQ US
Treatment
- Lactulose for hepatic encephalopathy - titrate to 3-4 bowel movements per day
- Consider addition of Rifaximin based on team discussion
- Nutritional support - consider calorie count, high protein diet
- Discuss DVT prophylaxis (heparin for Cr clearance < 30) with team before ordering
Daily F/U
- Vitals
- Trend of LFTs, INR
- Calculate MELD score
- Assess ability to hold conversation, mental status
- Bowel movements if hepatic encephalopathy
- Patient understanding of progress and plan, and expectation for discharge - dispo plan
- Follow up with family if needed
Renal
Acute Renal Failure (ARF), Acute Kidney Injury (AKI)
Relevant questions
- Symptoms
- Change in urine output or appearance
- Change in weight or PO intake
- Change in medications? New or same medications with dose changes
- Any change in mental status?
- Known creatinine baseline and dry weight
- If dialysis patient - who is their nephrologist? Adherent with HD? Last session?
Focused Exam
- Vital signs
- Volume status - JVD, HJR, edema
- Mental status - are they uremic? (confused, itchy, sleepy)
- If HD patient - fistula site look okay? Palpable thrill?
Data
-
Electrolytes to assess bicarb, Na, K, BUN, Cr
- AKI is defined as increase in Cr ~30% from baseline
-
EKG - especially if hyperK
- CBC
- Consider: urine lytes since you can use to calculate FeNa here (if not on loop diuretics)
- Intake/output
Treatment
- HOLD nephrotoxic medications - includes ACEi, NSAIDs
- Hydration - discuss with team based on assessed volume status
- Generally ok to continue DVT prophylaxis (heparin for Cr clearance < 30)
Daily F/U
- Vitals
- Daily creatinine - trend for improvement/back to baseline
- Urine output
- Patient understanding of progress and plan, and expectation for discharge
- Follow up with family and with PCP for recheck if needed
Acid/Base
Initial Approach
- Look at the pH. Whichever side of 7.4 the pH is on, the process that caused it to shift to that side is the primary disorder (i.e. acidosis or alkalosis). This is because the body never fully compensates for the primary acid-base disorder
- Calculate the anion gap. Look at the compensation. For a metabolic process the pCO2 should increase (metabolic alkalosis) or decrease (metabolic acidosis). For a respiratory process, the bicarbonate should increase (respiratory acidosis) or decrease (respiratory alkalosis)

Focused Exam
- Vital signs
- Respiratory status - respiratory rate? Retaining CO2?
- Urine appearance if available, output
Data
- BMP
- VBG
| Disorder | pH | pCO₂ | HCO₃⁻ | Clinical examples |
|---|---|---|---|---|
| Respiratory and metabolic acidosis | Very low | ↑ | Lower than expected | Cardiopulmonary arrest, cerebrovascular accident and renal failure |
| Respiratory and metabolic alkalosis | Very high | ↓ | Higher than expected | Congestive cardiac failure and vomiting, diuretic therapy and liver failure |
| Metabolic acidosis and respiratory alkalosis | ≈7.45 | Lower than expected | ↓ | Salicylate overdose, septic shock, sepsis and renal failure |
| Metabolic alkalosis and respiratory acidosis | ≈7.45 | Higher than expected | ↑ | Diuretic therapy or vomiting and emphysema |
| Metabolic acidosis and metabolic alkalosis | ≈7.45 | → | → | Lactic acidosis or diabetic ketoacidosis and vomiting |
| Triple disorder: mixed metabolic acidosis and alkalosis plus respiratory alkalosis or acidosis | Variable | Variable | Variable | Renal failure, vomiting and congestive cardiac failure |
Treatment
- Focused on underlying cause - discuss plan with team
Daily F/U
- Vitals
- Respiratory status - off of NIPPV? Or set up with home CPAP?
- Renal function - back at baseline?
- Clarify follow-up plan with patient and family
Hypertension
Relevant questions
- Symptoms: Headache, chest pain, palpitations, lightheadedness/syncope, abdominal pain
- Any medications for blood pressure? Have they changed at all?
- Changes to diet or activity level? Increased weight? Family history of hypertension?
- Do they know normal blood pressures for them
Focused Exam
- Vital signs
- Cardiac - murmurs, carotid bruit
- Abdominal - bruits, palpable mass
- Extremities - edema, pulses
- Fundoscopic exam if possible
Data
- EKG
- Electrolytes to assess bicarb, K, BUN, Cr
- CBC
- TSH reflex, cholesterol fractionation
- Urinalysis
Treatment
-
Step 1: Rule out hypertensive emergency (ie SBP>180 or DBP>120 AND end-organ damage
- (AMS/encephalopathy, visual changes, SOB, angina/ACS, renal damage, aortic dissection, CVA/ICH, acute CHF).
- If symptomatic, should get EKG, trop, BMP, and UA for proteinuria. Typically need to initiate BP drip (nitro, nicardipine, etc.) and go to Cardiac ICU.
-
Step 2: Treat anxiety, pain, look at home meds and/or meds received for the day.
-
Step 3: Per 2017 ACC/AHA guidelines, do not treat hypertensive urgency (aka asymptomatic elevated BP without end organ damage) with IV meds.
- Ideally: increase or restart chronic BP meds (but may get pushback)
- If necessary, can give PRN labetalol (5-10 mg IV)
- Alternative agent is hydralazine (5-10 mg IV) but generally not recommended due to unpredictable and prolonged antihypertensive effects
-
Typically, you want gradual MAP reduction by 20-30% over 24 hours if hypertensive urgency or over 2-4 hours in HTN emergency
-
Good oral antihypertensives
- Initial therapy ideally with ACEi/ARB or dihydropyridine CCB (ie Amlodipine), consider thiazide diuretic, chlorthalidone (ALLHAT)
- Base therapy decision on comorbid conditions and degree of hypertension on discussion with team if starting antihypertensives (or adding new ones)
- JNC8 recommends maximizing first antihypertensive before adding another agent
-
DVT prophylaxis (heparin for Cr clearance < 30)
Daily F/U
- Vitals and 02 sat
- Adequacy of BP control with oral medications
- Ability to obtain/take medications outpatient
- Patient understanding of progress and plan, and expectation for discharge
Infectious Disease
Sepsis
Relevant questions
-
Symptoms
-
Any focal symptoms
i. Urine changes? Color, frequency, pain, volume
ii. Cough, shortness of breath, sputum
iii. Congestion, sore throat, ear pain, sinus pain
iv. Abdominal pain, diarrhea, nausea/vomiting
v. Rash, swelling, pain
-
Syncope, lightheadedness
-
-
Any exposures?
- Sick contacts
- Prior history?
- Previous infections with emphasis on resistant organisms in the past
- IV drug use or other substance use
- Setting: from home or nursing home. Recent hospitalization
Focused Exam
- Vital signs and pulse ox
- Able to speak in complete sentences?
- Skin - rashes, edema
- Cardiac - new murmur
- Abdominal - pain, distension
- Back – palpate spine
- Lungs-Breath sounds, Air Exchange, focal findings
Data
- CXR on admission and with clinical change
- EKG
- Electrolytes to assess bicarb, K, BUN, Cr and glucose
- CBC
- Blood cultures
- Urinalysis (urine culture must be ordered separately)
- RPP
- Lactate
- Consider echocardiogram if suspicion for endocarditis - d/w team
- Consider c-diff or stool studies depending on symptoms, antibiotic exposure
Treatment
- Vancomycin 15mg/kg q12h - adjust based on renal function
- Zosyn 3.375 or 4.5 mg q6h - also adjust based on renal function
- Narrow antibiotics after pathogen determined
- Fluid resuscitation with LR preferentially - goal MAP > 60 at least, so if not there/improving after 3-4 liters would consider escalating care
- DVT prophylaxis (heparin for Cr clearance < 30)
Daily F/U
- Vitals and 02 sat
- Testing results - do you have a source?
- Day of hospitalization and course of antibiotics
- Need for further reimaging
- Patient understanding of progress and plan, and expectation for discharge
- Follow up with family if needed
Acute Cystitis
Relevant questions
-
Symptoms
- Pain with urination
- Increased frequency of urination
- Nausea/vomiting, inability to tolerate PO intake
-
Any prior history?
- What has worked in the past? On chronic suppression?
- Foley catheter?
-
Setting-from home or nursing home
Focused Exam
- Vital signs
- Abdominal exam - suprapubic tenderness, CVA tenderness
Data
- Urinalysis, urine culture
- Electrolytes to assess bicarb, K, BUN, Cr and glucose
- CBC
Treatment
- Do NOT treat if asymptomatic! Review exceptions.
-
Antibiotics - consider looking at our antibiogram and patient's prior UTIs if any
- PO options: Nitrofurantoin (definitely do not use if eGFR <30, cautious with 30-60), Levofloxacin, Ciprofloxacin, Cephalexin
- IV: Ceftriaxone, Zosyn, Levofloxacin, Meropenem if prior hx of ESBL
-
DVT prophylaxis (heparin for Cr clearance < 30)
Daily F/U
- Vitals
- Day of hospitalization and course of antibiotics
- Need for further reimaging or outpatient follow-up
- Patient understanding of progress and plan, and expectation for discharge
- Follow up with family if needed
Neurology
Encephalopathy
Relevant questions
-
Symptoms
- Quantify length of time over which symptoms developed
- Fevers, rashes, other infectious symptoms?
- Change in PO intake, urine output
- Abnormal movements or episodes of LOC?
-
Ask family/NH staff for collateral information
- Concerns? Change over time? Ability to care for self at home? Sick contacts?
- Baseline function
- Medication changes?
- Setting - from home or nursing home
Focused Exam
- Vital signs
- Neurologic exam
- Mental status assessment
Data
- BMP, LFTs, ammonia
- CBC
- VBG
-
Infectious testing: urinalysis (+ culture if suggestive of UTI), blood culture, CXR
- Consider LP, particularly if febrile
-
Urine tox screen
- Thyroid, serum osm tests. Consider B12, cortisol
- CT Brain non-contrast to start
- Further work-up to consider (often with Neuro input): MRI brain, EEG
Treatment
- Depends on etiology
- Consider seroquel, haldol only prn for severe agitation
- Thiamine for patients with hx of alcohol abuse, severe malnutrition
- DVT prophylaxis (heparin for Cr clearance < 30)
Daily F/U
- Vitals
- Improvement in mental status?
- Need for further workup/consultants on board?
- Patient/family understanding of progress and plan, and expectation for discharge
Endocrinology
Diabetes Mellitus
Relevant questions
-
Symptoms
- Do they know what their glucose has been recently? Highs or lows?
- Do they have symptoms with highs and lows?
- Any abdominal pain, nausea/vomiting, lightheadedness, clamminess?
- Change in diet?
- Home glucose - device monitoring levels/log?
-
Has there been a recent change to insulin?
- Have they been in the hospital for problems with diabetes? Recently?
- Inability to get or take medications
- Setting - from home or nursing home
Focused Exam
- Vital signs
- Fingerstick glucose
- Basic neuro assessment - are they mentating appropriately
- Abdominal exam
Data
- Fingerstick glucose TID AC and QHS
- Electrolytes to assess bicarb, K, BUN, Cr and glucose
- Hemoglobin A1c if no recent one available
Treatment
Endotool protocol is used in the hospital. Remember to follow-up with glucose changes.
-
Insulin - adjust daily based on previous 24 hours insulin requirements
- Total Daily Dose (TDD) = sum total of all insulin scheduled to be given during a 24 hr period
- Initial TDD for type 2 diabetes: 0.3 – 0.4 units/kg/day. For type 1, use 0.3 – 0.8 units/kg/day
-
50% of TDD is given as basal insulin, 50% as rapid- acting insulin distributed across 3 meals
- Basal Insulin = long acting insulin required to maintain normal BG overnight and while NPO
- Mealtime Bolus Insulin = rapid-acting insulin used to cover meal-induced rise in glucose
-
Continue basal insulin (glargine/Lantus, NPH) at outpatient doses or cut in 1⁄2 if NPO
-
Goals: avoid hypoglycemia, severe hyperglycemia, and electrolyte abnormalities
- Critically ill patients: < 140 mg/dl, tight control 80- 110 mg/dl may be associated with increased mortality
- Non–critically ill patients: premeal BG levels between 90–130 mg/dl, all fasting BG < 180 mg/dl
-
Oral medications: hold metformin and sulfonylureas upon admission in most cases
Daily F/U
- Vitals
- Adequacy of glucose control
- Plan for outpatient follow-up
- Patient/family understanding of plan
Disclaimer
Always verify with your superiors before taking action based on this guide. The information is intended to help, but not to dictate your course of work. Always use critical judgment and your clinical knowledge skills. This guide will be constantly revised and updated according to evidence-based medicine.
Common Medications: Quick Reference
A practical guide to frequently used inpatient medications organized by therapeutic category. All dosing reflects standard adult hospital practice; always verify with institutional protocols and patient-specific factors (renal function, hepatic disease, drug interactions).
Bowel Regimen
Constipation is preventable. Start bowel medications proactively in all patients on opioids.
| Drug | Starting Dose | Onset | Indication | Notes |
|---|---|---|---|---|
| Docusate | 100mg PO BID | 24–72h | Stool softener for mild constipation | Often combined with other agents; minimal efficacy alone |
| Miralax (polyethylene glycol) | 17g PO daily–BID | 1–4 days | First-line osmotic laxative | Very safe, well-tolerated; increase as needed |
| Magnesium hydroxide (Milk of Magnesia) | 30–60mL PO | 6–12h | Rapid osmotic laxative | Avoid in renal failure; faster than Miralax |
| Magnesium citrate | 150mL PO | 30min–2h | Rapid bowel evacuation | Very fast; use when urgent |
| Lactulose | 10–30cc PO q4–6h | 1–2h | Osmotic laxative | Causes bloating/flatulence; less tolerated |
| Senna | 2–4 tablets PO daily–BID | 6–12h | Stimulant laxative | Natural alternative; safe for chronic use |
| Bisacodyl | 10–30mg PO or PR | 6–10h | Stimulant (oral or rectal) | Rectal suppository faster onset |
| GoLytely (PEG solution) | 4L PO or NG tube | 1–2h | Aggressive bowel prep | For severe impaction; very potent |
| Methylnaltrexone (Relistor) | 8–12mg SC every other day | 30–60min | Refractory opioid-induced constipation | Peripheral antagonist; preserves analgesia |
Opioid-Induced Constipation Protocol
Always initiate bowel regimen when starting opioids. Standard approach: Miralax + Senna. Escalate to stronger agents if ineffective after 48–72h. Add methylnaltrexone if refractory to standard therapy.
Antiemetics
Choose antiemetic based on etiology. Always investigate the cause before masking nausea.
| Drug | Starting Dose | Frequency | Mechanism | Notes |
|---|---|---|---|---|
| Ondansetron | 4–8mg | PO/IV q8h | 5-HT3 antagonist | Check QTc; avoid if QTc >500; good for post-op nausea |
| Promethazine | 25mg IV or 50mg PO | q4–6h | H1 antagonist + anticholinergic | Sedating; risk of extrapyramidal effects; IV push risk of necrosis |
| Metoclopramide | 10mg | PO/IV q6h | Dopamine antagonist + prokinetic | Check QTc; avoid in mechanical obstruction |
| Prochlorperazine | 5–10mg | IV q4–6h | Dopamine antagonist | Risk of dystonia, QTc prolongation |
| Scopolamine patch | 1 patch | Q72h (behind ear) | Anticholinergic | Effective for motion sickness; risk of urinary retention |
Assess Before Treating
Do not reflexively prescribe antiemetics. Nausea from obstruction, perforation, or intracranial pathology masked by antiemetics delays diagnosis. Always obtain focused exam and consider imaging.
Pain Management: Non-Opioid Analgesics
Start with non-opioid options. Opioids should be last resort.
| Drug | Starting Dose | Frequency | Indication | Cautions |
|---|---|---|---|---|
| Acetaminophen | 650mg | PO/PR q6h (max 4g/day) | Mild-moderate pain, fever | Avoid in active liver disease; monitor total daily dose |
| Ibuprofen | 200–800mg | PO q6h | Mild-moderate pain, inflammation | Avoid GI bleed, GERD, ACS, CHF, AKI |
| Naproxen | 500mg | PO q12h | Mild-moderate pain | Avoid GI bleed, GERD, ACS, CHF, AKI; longer duration |
| Ketorolac | 30mg | IV/PO q6h (max 5 days) | Moderate acute pain | Short-acting only; avoid GI bleed, GERD, renal disease |
| Lidocaine patch | 1–3 patches | Apply q12h | Localized neuropathic pain | Maximum 3 patches simultaneously; safe, low systemic absorption |
| Topical diclofenac gel | Apply liberally | TID–QID | Joint/muscle pain | Minimal systemic absorption; good for localized pain |
Multimodal Analgesia
Combine non-opioid agents (acetaminophen + NSAID + topical) with non-pharmacologic strategies (positioning, ice/heat, elevation) before resorting to opioids.
Pain Management: Opioid Analgesics
Use lowest effective dose for shortest duration. Prefer PO when possible. Always obtain baseline pain assessment.
| Drug | Starting Dose | Duration | Route | Notes |
|---|---|---|---|---|
| Tramadol | 50mg | q4–6h | PO | Lower seizure threshold; avoid in seizure disorder |
| Hydrocodone/APAP | 5–10mg/325mg | q4–6h | PO | Monitor total acetaminophen dose; max 4g/day |
| Oxycodone | 5mg | q4–6h | PO | Short-acting; good for acute pain; more euphoria than other agents |
| Morphine (immediate-release) | 15–30mg | q4h | PO | Standard opioid; caution in renal failure (accumulation) |
| Morphine | 2–4mg | q4h | IV | Slower onset than IV; monitor respiratory depression |
| Hydromorphone (Dilaudid) | 1–2mg | q4–6h | PO | Potent; 1mg PO = ~2mg oxycodone |
| Hydromorphone (Dilaudid) | 1mg (0.5mg if elderly) | q4–6h | IV | Shorter duration than morphine; use low doses in frail |
| Fentanyl | 0.1mg | q1–2h | IV | Very potent; rapid onset; reserved for severe acute pain |
Opioid Conversion Table
When switching formulations, convert to morphine equivalents (MEQ) first, then calculate new agent dose.
| Drug | Route | Conversion to MEQ | Duration |
|---|---|---|---|
| Morphine | IV (10mg) | 1 MEQ | 4h |
| Morphine | PO (30mg) | 1 MEQ | 4h |
| Hydrocodone | PO (30mg) | 1 MEQ | 4h |
| Oxycodone | PO (20mg) | 1 MEQ | 4h |
| Oxycodone | IV (10mg) | 1 MEQ | 4h |
| Tramadol | IV (100mg) | 1 MEQ | 4h |
| Tramadol | PO (120mg) | 1 MEQ | 4h |
| Hydromorphone | IV (1.5mg) | 1 MEQ | 4h |
| Hydromorphone | PO (7.5mg) | 1 MEQ | 4h |
| Fentanyl | IV (0.1mg) | 1 MEQ | 1–2h |
Example conversion: Patient on Hydromorphone 1mg IV q4h = 0.67 MEQ per dose. If switching to PO Oxycodone, equivalent dose = 0.67 MEQ × 20mg/MEQ = 13.4mg q4h (round to 10–15mg).
Opioid Prescribing Safety
Write one-time orders rather than standing schedules. Reassess need at each patient interaction. Keep naloxone at bedside for all opioid patients. Monitor for respiratory depression, oversedation, and constipation.
Opioid Reversal
| Drug | Dose | Route | Duration | Notes |
|---|---|---|---|---|
| Naloxone (Narcan) | 0.4–0.8mg | IV push | 30–90min | Repeat q2–3min if needed; short duration (may need repeat dosing); watch for withdrawal |
Opioid Withdrawal
Naloxone precipitates acute withdrawal (agitation, diaphoresis, pain). Consider half-doses in opioid-dependent patients. Have benzodiazepines at bedside.
Antibiotics: Common Inpatient Agents
Always use local antibiogram and culture results to guide therapy. Listed here are empiric first-line agents.
| Drug | Starting Dose | Frequency | Spectrum | Common Indications | Cautions |
|---|---|---|---|---|---|
| Ceftriaxone | 1g | IV q12h | 3rd-gen cephalosporin (gram-neg, some gram-pos) | Community-acquired pneumonia, UTI, meningitis | Avoid if cephalosporin allergy; diarrhea risk |
| Cefepime | 1–2g | IV q8–12h | 4th-gen cephalosporin (broader gram-neg) | Hospital-acquired pneumonia, Pseudomonas concern | Better gram-neg than ceftriaxone; risk of encephalopathy with high doses |
| Piperacillin-tazobactam | 3.375–4.5g | IV q6h | Broad-spectrum (anaerobes, Pseudomonas) | Complicated intra-abdominal, polymicrobial | Monitor for rash, phlebitis; need renal dosing |
| Vancomycin | 15–20mg/kg | IV q8–12h | Gram-positive (MRSA coverage) | MRSA pneumonia/bacteremia, endocarditis | Monitor trough levels (goal 15–20); nephrotoxic; ototoxic |
| Azithromycin | 500mg loading | PO/IV daily | Macrolide (atypical organisms) | Atypical pneumonia (Chlamydia, Mycoplasma) | GI side effects; QTc prolongation |
| Fluoroquinolone (levofloxacin) | 750mg | PO/IV daily | Broad-spectrum (gram-neg + some gram-pos) | Community-acquired pneumonia, UTI | Tendon rupture, peripheral neuropathy, QTc prolongation risk |
| Trimethoprim-sulfamethoxazole | 1–2DS tablets or 5mg/kg TMP | PO/IV BID | Gram-pos + gram-neg + anaerobes | UTI, PCP prophylaxis | Rash, hyperkalemia, Stevens-Johnson syndrome risk |
| Metronidazole | 500mg | PO/IV q8h | Anaerobes, parasites | Anaerobic infections, C. difficile, trichomoniasis | Metallic taste, disulfiram reaction with alcohol |
| Clindamycin | 300–600mg | PO/IV q6–8h | Gram-pos + anaerobes | Streptococcal infections, aspiration pneumonia | C. difficile diarrhea risk; rash |
Empiric Sepsis Coverage
Standard empiric regimen: Ceftriaxone or cefepime + vancomycin (add gentamicin if Pseudomonas high risk). De-escalate once sensitivities available.
Antihypertensives: Acute and Chronic Control
Oral Agents (for hypertensive urgency, chronic control)
| Drug | Starting Dose | Frequency | Class | Mechanism | Cautions |
|---|---|---|---|---|---|
| Metoprolol | 25–50mg | PO BID | Beta-blocker | AV nodal blockade, decreased cardiac output | Avoid in hypotension, bradycardia, asthma/COPD |
| Carvedilol | 3.125–6.25mg | PO BID | Alpha/beta-blocker | Combined alpha and beta effects | Avoid if HR <55; may worsen CHF acutely |
| Diltiazem | 30–120mg | PO TID–QID | Calcium channel blocker | AV nodal blockade | Avoid in hypotension, bradycardia, acute CHF |
| Amlodipine | 2.5–5mg | PO daily | Calcium channel blocker (dihydropyridine) | Peripheral vasodilation | Slower onset; good for chronic control; ankle edema |
| Lisinopril | 5–10mg | PO daily | ACE inhibitor | Renin-angiotensin blockade | Avoid in hyperkalemia, AKI; dry cough common |
| Captopril | 12.5–25mg | PO TID | ACE inhibitor | Renin-angiotensin blockade | Fastest onset of ACE inhibitors; caution in AKI |
| Clonidine | 0.1–0.3mg | PO BID | Central alpha-2 agonist | Sympathetic inhibition | Reflex tachycardia; rebound HTN if discontinued abruptly |
| Hydralazine | 10–25mg | PO QID | Vasodilator | Direct vasodilation | Reflex tachycardia; lupus-like syndrome with chronic use |
Intravenous Agents (for more rapid control)
| Drug | Dosing | Route | Onset | Mechanism | Cautions |
|---|---|---|---|---|---|
| Labetalol | 10–20mg IV bolus; repeat q4–6h | IV push | 5–10min | Alpha/beta-blocker | Avoid in acute CHF, bradycardia; reflex tachycardia rare |
| Hydralazine | 10–20mg IV q6h | IV push | 10–20min | Direct vasodilation | Reflex tachycardia; caution in CAD, MI |
| Nicardipine | 5–15mcg/kg/min | IV infusion (titrate) | 5–10min | Calcium channel blocker | Titrable; good for gradual control; risk of reflex tachycardia |
| Esmolol | 50–300mcg/kg/min | IV infusion (titrate) | 1–5min | Ultra-short-acting beta-blocker | Very rapid titration and reversal; useful if trial needed |
| Nitroglycerin | 5–400mcg/min | IV infusion (titrate) | 1–3min | Nitrate (vasodilation + preload reduction) | Use for ACS + HTN; causes tachyphylaxis; avoid in RV MI |
| Nitroprusside | 0.5–10mcg/kg/min | IV infusion (titrate) | Immediate | Dual vasodilation (arterial + venous) | Risk of cyanide/thiocyanate toxicity; avoid prolonged use |
HTN Management Goals
Avoid aggressive reduction in asymptomatic patients. Target gradual reduction (10–15mmHg per hour). Do not drop mean arterial pressure >30% or SBP >40mmHg in first hour (stroke/AKI risk).
Cardiac Medications
Beta-Blockers and Rate-Control Agents
| Drug | Starting Dose | Frequency | Route | Indication | Notes |
|---|---|---|---|---|---|
| Metoprolol | 5–10mg | q4–6h | IV (acute); 25–50mg | AF-RVR, ACS, HTN | Cardioselective; caution in asthma/COPD |
| Diltiazem | 10mg bolus; 5–10mg/h drip | q4–6h (bolus) or continuous | IV/PO | AF-RVR (rate control), HTN | Negative inotrope; caution in CHF |
| Esmolol | 50–300mcg/kg/min drip | Continuous (titrate) | IV | Acute AF-RVR, intraoperative tachycardia | Ultra-short-acting; rapid reversal |
| Digoxin | 0.5–1mg loading | Single or divided | PO/IV | AF-RVR in CHF, narrow therapeutic window | Narrow therapeutic window; monitor levels (goal 0.8–2.0ng/mL) |
Antiarrhythmics
| Drug | Starting Dose | Frequency | Route | Mechanism | Cautions |
|---|---|---|---|---|---|
| Amiodarone | 150mg bolus over 10min, then 360mg over 6h | Variable drip | IV infusion | Class III antiarrhythmic (multiple mechanisms) | Decreases rate + converts rhythm; risk of QTc prolongation, bradycardia |
| Flecainide | 100–200mg | BID | PO | Class IC antiarrhythmic | Avoid in structural heart disease (risk of proarrhythmia); requires cardiology |
| Sotalol | 80–160mg | BID | PO | Class III antiarrhythmic + beta-blocker | Risk of torsades; monitor QTc, K, Mg; requires cardiology |
ACE Inhibitors and Other Cardiac Agents
| Drug | Starting Dose | Frequency | Indication | Notes |
|---|---|---|---|---|
| Lisinopril | 5–10mg | PO daily | CHF, post-MI, HTN | Vasodilation + reduced afterload; hyperkalemia risk |
| Enalapril | 2.5–5mg | PO BID | CHF, post-MI, HTN | Longer-acting than captopril; oral option |
| Carvedilol | 3.125–6.25mg | PO BID | CHF (evidence-based) | Improves EF in systolic CHF; start low in CHF |
| Furosemide | 20–80mg | PO/IV daily–BID | CHF, pulmonary edema, fluid overload | Monitor K, Cr; can cause hypokalemia |
| Nitroglycerin SL | 0.3–0.6mg | q5min PRN | Acute angina, ACS, pulmonary edema | Avoid in RV MI (preload-dependent); tachyphylaxis |
Pulmonary Medications
Bronchodilators
| Drug | Starting Dose | Frequency | Route | Indication | Notes |
|---|---|---|---|---|---|
| Albuterol | 2.5–5mg | q4–6h PRN | Nebulized or inhaler | Asthma/COPD exacerbation, bronchospasm | Beta-2 agonist; risk of tremor, tachycardia |
| Ipratropium | 0.5mg | q6h | Nebulized (combo with albuterol) | COPD exacerbation (synergistic with albuterol) | Anticholinergic; longer duration than albuterol |
| Levalbuterol | 0.63–1.25mg | q8h | Nebulized | Asthma/COPD exacerbation (alternative to albuterol) | R-isomer of albuterol; less tremor/tachycardia |
| Theophylline | 300mg | BID | PO (sustained-release) | Chronic COPD (rarely used now) | Narrow therapeutic window; monitor levels |
Inhaled Corticosteroids
| Drug | Dosing | Frequency | Indication | Notes |
|---|---|---|---|---|
| Fluticasone/Salmeterol (Advair) | 1–2 puffs | BID | Chronic asthma/COPD maintenance | Combination ICS + LABA; do not use for acute exacerbation |
| Budesonide/Formoterol (Symbicort) | 1–2 puffs | BID | Chronic asthma maintenance | ICS + LABA; can use as maintenance + reliever |
Systemic Corticosteroids (for acute exacerbation)
| Drug | Starting Dose | Frequency | Route | Indication | Notes |
|---|---|---|---|---|---|
| Methylprednisolone | 40–125mg | q4–6h | IV | Acute asthma/COPD exacerbation | Rapid onset; reserve IV for severe exacerbation |
| Prednisone | 40–60mg | daily | PO | Mild-moderate exacerbation (outpatient) | Slower onset; adequate for less severe exacerbations |
Sedation and Agitation: Psychiatric Medications
Antipsychotics (for acute agitation/delirium)
| Drug | Starting Dose | Frequency | Route | Notes | Cautions |
|---|---|---|---|---|---|
| Haloperidol | 2–5mg (1mg elderly) | q4–6h | PO/IM/IV | Typical antipsychotic; rapid onset | QTc prolongation; monitor EKG; extrapyramidal side effects; max 20mg/day |
| Olanzapine | 2.5–5mg | q6h | PO/IM | Atypical; lower dystonia risk | Metabolic syndrome risk; monitor QTc |
| Quetiapine | 12.5–25mg | q6h | PO | Atypical; minimal movement disorder | Lower antipsychotic potency; often used at low doses |
| Risperidone | 0.5–1mg | BID | PO | Atypical; effective antipsychotic | Risk of prolactin elevation; orthostasis |
| Ziprasidone | 10mg | IM q4–6h | IM (IV not available in US) | Atypical; short-acting IM option | Monitor QTc; lower weight gain than others |
| Aripiprazole | 2–5mg | daily–BID | PO/IM | Atypical; D2 partial agonist | Use if QTc >500; lower metabolic effects |
Benzodiazepines (Use Cautiously—Delirium Risk)
| Drug | Starting Dose | Frequency | Route | Indication | Cautions |
|---|---|---|---|---|---|
| Lorazepam | 1–2mg | q4–6h | PO/IV | Anxiety, alcohol withdrawal, seizure | Short-acting; risk of dependence, delirium in elderly |
| Alprazolam | 0.25–0.5mg | q8h | PO | Anxiety (avoid—no better than others) | Long-acting; accumulates in elderly and renal failure |
| Midazolam | 0.15mg/kg | Single or repeated | IV/IM | Acute seizure, severe anxiety | Ultra-short-acting; risk of respiratory depression |
Alternatives to Benzodiazepines
| Drug | Starting Dose | Frequency | Route | Indication | Notes |
|---|---|---|---|---|---|
| Hydroxyzine | 50–100mg | q4–6h | PO/IV | Anxiety, agitation | Non-controlled alternative to benzos; antihistamine |
| Buspirone | 7.5–15mg | BID | PO | Chronic anxiety (not acute) | Slow onset; takes days to weeks; no sedation |
Anticoagulation and DVT Prophylaxis
DVT Prophylaxis (Mechanical + Pharmacologic)
| Drug | Starting Dose | Frequency | Indication | Cautions |
|---|---|---|---|---|
| Enoxaparin | 40mg | SC daily | DVT prophylaxis (hospitalized patients) | Adjust dose if CrCl <30; monitor for HIT |
| Fondaparinux | 5–10mg (weight-based) | SC daily | DVT prophylaxis (alternative to heparin) | Adjust for CrCl; avoid if CrCl <20 |
| Unfractionated heparin | 5,000 units | SC BID–TID | DVT prophylaxis (renal failure preference) | Monitor aPTT if higher doses; requires baseline platelet count |
Therapeutic Anticoagulation (for VTE, AF, mechanical valve)
| Drug | Loading Dose | Maintenance | Route | Cautions |
|---|---|---|---|---|
| Unfractionated heparin | 80 units/kg bolus | 18 units/kg/h infusion (titrate to aPTT 60–85) | IV | Monitor aPTT q6h initially; HIT risk; reversal with protamine |
| Enoxaparin | 1mg/kg x1 | 1mg/kg q12h or 1.5mg/kg daily | SC | Adjust for CrCl; monitor anti-Xa levels if needed |
| Apixaban | 10mg x1 | 5mg BID | PO | Direct Factor Xa inhibitor; no monitoring; renal adjustment |
| Rivaroxaban | 15–20mg x1 (with food) | 20mg daily (with food) | PO | Direct Factor Xa inhibitor; no monitoring |
| Dabigatran | 150mg x1 | 150mg BID | PO | Direct thrombin inhibitor; no monitoring; renal adjustment |
| Warfarin | 5–10mg | Titrate to INR 2–3 (goal varies by indication) | PO | Monitor INR; many interactions; slow onset/offset; baseline PT/INR |
Reversal Agents
| Agent | Bleeding Type | Anticoagulant | Dose | Notes |
|---|---|---|---|---|
| Fresh frozen plasma (FFP) | Major | Warfarin, UFH | 10–15mL/kg | Non-specific; volume risk; slower reversal |
| Prothrombin complex (PCC) | Major GI/CNS | Warfarin | 25–50 units/kg | Faster warfarin reversal than FFP; preferred |
| Vitamin K1 | Major | Warfarin | 2.5–5mg IV | Slow onset (12–24h); use with PCC for rapid reversal |
| Idarucizumab | Major | Dabigatran | 5g IV (two 2.5g infusions) | Specific reversal; rapid; expensive |
| Andexanet alpha | Major | Apixaban, rivaroxaban | Weight/age-based bolus + infusion | Specific Factor Xa reversal; consider cost/access |
| Protamine sulfate | Major | UFH | 1mg per 100 units UFH (max 50mg) | For heparin reversal; rapid onset |
Anticoagulation Reversal
Major bleeding on anticoagulation requires immediate reversal. Have reversal agents in mind for each agent. Contact pharmacy/hematology if unsure. Do not delay reversal in life-threatening bleeding.
Electrolyte Replacement
| Electrolyte | Deficiency | Starting Dose | Route | Target | Monitoring |
|---|---|---|---|---|---|
| Potassium | Hypokalemia (K <3.5) | 10–20 mEq | PO/IV (slow if IV) | K 3.5–5.0 | Daily K, EKG if <3.0 |
| Magnesium | Hypomagnesemia (Mg <1.7) | 1–2g | PO/IV | Mg 1.7–2.2 | Daily Mg; adjust for renal function |
| Calcium | Hypocalcemia (Ca <8.5) | 500–1000mg | PO/IV (calcium gluconate for IV) | Ca 8.5–10.5 | Daily Ca; ionized Ca if critical |
| Sodium | Hyponatremia (Na <130) | Varies by acuity/severity | IV hypertonic saline (3%) | Na >130 (slowly to avoid osmotic demyelination) | Frequent Na checks; max correction 4–6 mEq/L per 24h |
| Phosphate | Hypophosphatemia (P <2.5) | 10–20 mmol | PO/IV | P 2.5–4.5 | Monitor with K, Ca replacement |
Hyponatremia Correction
Overcorrection of sodium (>8–10 mEq/24h) risks osmotic demyelination syndrome (ODS). Correct slowly; target 4–6 mEq/24h increase unless acute symptomatic hyponatremia (<48h, seizures, LOC).
Immunizations (Inpatient)
| Vaccine | Indication | Timing | Route | Notes |
|---|---|---|---|---|
| Influenza (inactivated) | Annual; all patients | Once per season | IM | Exclude egg allergy |
| Pneumococcal (PPSV23, PCV20) | Age ≥65 or chronic disease | Single or sequenced per guidelines | IM | Guidelines change; check current CDC recommendations |
| Tetanus/diphtheria/pertussis (Tdap) | If ≥10y since last | Single dose | IM | Repeat q10y |
| Meningococcal | College students, asplenic patients | Per risk | IM | Various formulations; check indication |
Summary: Medication Safety Principles
- Always verify renal function before dosing (many drugs renally eliminated; adjust if CrCl <60)
- Check drug interactions (especially with warfarin, statins, ACE inhibitors)
- Monitor therapeutic levels when applicable (vancomycin, digoxin, phenytoin, theophylline)
- Reassess need at each patient interaction (avoid unnecessary continuation)
- Know your patient's allergies (especially beta-lactams, sulfonamides)
- Document rationale for high-risk drugs (opioids, benzodiazepines, anticoagulants)
- Always de-escalate from broad-spectrum antibiotics once sensitivities available
Disclaimer: This guide is for educational purposes. Always follow institutional protocols, verify doses with primary sources, and consult pharmacy for specific patient scenarios.
On-Call Pearls: Quick Reference Guide
A rapid-access clinical resource for overnight hospital calls and acute clinical scenarios. This guide emphasizes rapid assessment, red flag identification, and evidence-based interventions for the busy resident.
Pain Management
Every pain complaint requires structured evaluation before jumping to narcotics.
Initial Assessment Framework
Before prescribing, always determine:
- Nature of pain: Is this new acute pain or exacerbation of chronic pain?
- Characterization: Use PQRST (Provocation, Quality, Radiation, Severity, Timing)
- Red flags requiring urgent intervention:
- Fever with new pain (infection/sepsis)
- Focal neurological deficits (CVA, cord compression)
- Loss of consciousness
- Hemodynamic instability
Red Flag Presentation
New acute pain with fever, focal deficits, or hemodynamic changes requires urgent evaluation. Do not mask symptoms with pain medications until serious causes are excluded.
Non-Opioid Analgesics (First-Line)
Always attempt non-pharmacologic and non-opioid approaches before opioids.
| Medication | Dosing | Indications | Cautions |
|---|---|---|---|
| Lidocaine patches | Apply topically q12h | Localized neuropathic, musculoskeletal pain | Max 3 patches simultaneously |
| Acetaminophen | 650mg PO/PR q6h | Mild-moderate pain, fever | Max 4g/day; avoid active liver disease |
| Ibuprofen | 200–800mg PO q6h | Mild-moderate pain, inflammation | Avoid GI bleed, GERD, ACS, CHF, AKI |
| Naproxen | 500mg PO q12h | Mild-moderate pain | Avoid GI bleed, GERD, ACS, CHF, AKI |
| Ketorolac | 30mg IV/PO q6h (max 5 days) | Moderate acute pain | Avoid GI bleed, GERD, ACS, CHF, AKI; short duration only |
Opioid Analgesics (When Necessary)
When opioids are indicated, use the lowest effective dose for the shortest duration. Prefer oral formulations when possible.
| Medication | Dosing | Duration | Notes |
|---|---|---|---|
| Tramadol | 50mg PO q4–6h | 4–6 hours | Use cautiously; lower seizure threshold |
| Hydrocodone/APAP | 5–10mg/325mg PO q4–6h | 4–6 hours | Watch total acetaminophen dose |
| Oxycodone | 5mg PO q4–6h | 4–6 hours | Short-acting, useful for acute pain |
| Morphine (IR) | 15–30mg PO q4h or 2–4mg IV q4h | 4 hours | Use lower IV doses in renal disease |
| Hydromorphone (Dilaudid) | 1mg IV q4–6h (0.5mg if elderly/frail) | 3–4 hours | Potent; appropriate for severe pain |
| Fentanyl | 0.1mg IV (onset 1–2 min) | 1–2 hours | Reserved for acute severe pain |
Opioid Prescribing Strategy
Write one-time orders rather than standing schedules when possible. Reassess need at every interaction. Always offer non-opioid alternatives first.
Respiratory Depression Risk
Monitor for respiratory depression and altered mental status, especially in elderly patients and those with underlying pulmonary disease. Keep Narcan at bedside.
Opioid Reversal
Naloxone (Narcan): 0.4mg IV; repeat q2–3min if needed. Watch for opioid withdrawal.
Opioid Conversion Reference
When switching between opioid formulations, convert to morphine equivalent first (MEQ), then calculate the new agent dose.
| Drug (Route) | IV Morphine Equivalent | PO Equivalent | Duration |
|---|---|---|---|
| Morphine (IV) | 10mg = 1 MEQ | 30mg PO | 4 hours |
| Hydrocodone (PO) | — | 30mg PO | 4 hours |
| Oxycodone (PO) | — | 20mg PO | 4 hours |
| Oxycodone (IV) | 10mg = 1 MEQ | — | 4 hours |
| Tramadol (IV/PO) | 100mg IV = 1 MEQ | 120mg PO | 4 hours |
| Hydromorphone (IV) | 1.5mg IV = 1 MEQ | 7.5mg PO | 4 hours |
| Fentanyl (IV) | 0.1mg = 1 MEQ | — | 1–2 hours |
Nausea and Vomiting
Nausea is a symptom, not a diagnosis. Always consider the underlying etiology before treating.
Differential Diagnosis Framework

Critical Assessment
Before administering antiemetics, obtain:
- Vital signs (fever, tachycardia, hypotension suggest serious pathology)
- Focused abdominal and neurological exam
- Consider stat imaging (CT abdomen/pelvis, CT head) if red flags present
- Check recent labs and medication list
Antiemetic Medications
| Drug | Dosing | Mechanism | Cautions |
|---|---|---|---|
| Ondansetron | 4–8mg PO/IV q8h | 5-HT3 antagonist | Check QTc; avoid if prolonged |
| Promethazine | 25mg IV or 50mg PO q4–6h | Anticholinergic + antihistamine | Sedating; caution in elderly; risk of necrosis if IV push extravasates |
| Metoclopramide | 10mg IV/PO q6h | Dopamine antagonist | Check QTc; avoid in bowel obstruction |
| Prochlorperazine | 5–10mg IV q4–6h | Dopamine antagonist | Monitor for dystonia, QTc prolongation |
Assessment Required
Do not reflexively prescribe antiemetics without evaluation. Masking symptoms may delay diagnosis of serious pathology (obstruction, GI perforation, CNS lesion).
Insomnia
Insomnia in hospitalized patients often reflects underlying disease or medication effects, not merely poor sleep hygiene.
Root Cause Identification
Before reaching for sedatives, investigate:
- Pain (undertreated analgesia is a major cause)
- Delirium (confusion/disorientation with insomnia suggests encephalopathy, not primary insomnia)
- Medication withdrawal (benzodiazepines, alcohol)
- Environmental factors (frequent vital signs, monitors, roommate)
- Circadian disruption (overhead lighting, frequent daytime sleeping)
Non-Pharmacologic Interventions
- Consolidate vital signs and lab work to minimize nighttime interruptions
- Dim lights after dusk; encourage daytime activity
- Address pain adequately
- Avoid sedating medications early in the morning (impairs neuro exam)
Sleep Medication Options
| Drug | Dosing | Notes |
|---|---|---|
| Melatonin | 3–9mg PO qhs | Natural, low risk; variable efficacy |
| Trazodone | 25–100mg PO qhs (start low) | Can cause orthostatic hypotension and priapism |
| Zolpidem | 5mg PO qhs | Extreme caution in elderly (fall risk, delirium) |
| Diphenhydramine | 25–50mg PO qhs | Use only in young, healthy patients; anticholinergic risks in elderly |
Benzodiazepines Contraindicated
Never use benzodiazepines for insomnia in hospitalized patients. Markedly increases delirium risk, falls, and respiratory depression. Reserve benzos only for seizure, severe anxiety, or withdrawal.
Anxiety
Anxiety can be a symptom of serious underlying illness. Always differentiate primary anxiety from secondary causes.
Red Flags: Anxiety Masking Critical Illness
- Anxiety + tachypnea: Suspect PE, pneumonia, sepsis, MI
- Anxiety + disorientation: Suspect hypoglycemia, delirium, hypoxia
- Anxiety + fever: Suspect sepsis, meningitis
- Anxiety + chest pain: Suspect ACS, PE, pneumothorax
Medication History
Carefully review home medications: - Is the patient on chronic benzodiazepines? If yes, holding them may cause withdrawal (tachycardia, tremor, agitation) - If withdrawal suspected, institute benzodiazepine replacement before acute anxiety treatment
Anxiolytic Options
| Drug | Dosing | Duration | Notes |
|---|---|---|---|
| Lorazepam | 1–2mg PO/IV q4–6h | 4–6 hours | Short-acting; monitor for over-sedation |
| Alprazolam | 0.25–0.5mg PO q8h | 6–8 hours | Longer-acting; avoid in renal failure |
| Hydroxyzine | 50–100mg PO/IV q4–6h | 6 hours | Non-controlled; good alternative to benzos |
Benzodiazepine Caution
Use short-acting benzodiazepines cautiously. Monitor for delirium, respiratory depression, and falls. Always rule out serious causes before treating anxiety pharmacologically.
Hypertension
Hypertension in hospitalized patients is usually reactive. Aggressive treatment can cause harm.
Initial Evaluation
Differentiate acute hypertensive urgency from hypertensive emergency:
- Hypertensive urgency: SBP/DBP >180/120 WITHOUT end-organ damage (asymptomatic)
- Hypertensive emergency: SBP/DBP >180/120 WITH end-organ symptoms
Red Flag Symptoms (Hypertensive Emergency)
- Chest pain or dyspnea
- Severe headache
- Vision changes or fundoscopic papilledema
- Focal neurological deficits
- Decreased urine output
- Signs of left ventricular failure (orthopnea, pulmonary edema)
Workup for Severe HTN
| Study | Purpose |
|---|---|
| EKG | Assess for ischemia, LVH |
| Troponin | Rule out ACS |
| CXR | Evaluate for pulmonary edema |
| Metabolic panel | Assess renal function, K |
| CBC with differential smear | Rule out hemolysis, thrombotic microangiopathy |
| Urinalysis | Check for proteinuria, RBC casts |
| Head CT | If altered mental status or neuro findings |
Antihypertensive Agents
Oral Agents (for hypertensive urgency, asymptomatic)
| Drug | Dosing | Mechanism | Cautions |
|---|---|---|---|
| Clonidine | 0.1–0.3mg PO | Central alpha-2 agonist | Reflex tachycardia; rebound HTN if stopped abruptly |
| Captopril | 25mg PO | ACE inhibitor | Caution in AKI; hyperkalemia risk |
| Carvedilol | 3.125–25mg PO | Combined alpha/beta-blocker | Avoid if HR <55; may worsen CHF acutely |
| Amlodipine | 2.5–10mg PO | Calcium channel blocker | Slower onset; good for chronic control |
Intravenous Agents (for more rapid control or hemodynamic instability)
| Drug | Dosing | Onset | Cautions |
|---|---|---|---|
| Labetalol | 10–20mg IV q4–6h | 5–10 min | Avoid in acute CHF, bradycardia |
| Hydralazine | 10–20mg IV q6h | 10–20 min | Reflex tachycardia; lupus-like syndrome with chronic use |
| Nicardipine | 5–15mcg/kg/min drip | 5–10 min | Titrable; good for rapid control |
| NTG drip | 5–400mcg/min | 1–3 min | Use for ACS + HTN; causes tachyphylaxis |
Treatment Goals
- Hypertensive urgency (asymptomatic, >180/120): Gradual reduction; target <160/100 over hours
- Hypertensive emergency (symptomatic): Controlled reduction; target 75% of admission BP initially
- Maximum safe reduction: Do not drop MAP >30% or SBP >40mmHg in first hour (risk of stroke, AKI)
Conservative Approach
Avoid aggressive BP lowering in asymptomatic patients. Most hypertension resolves with treatment of underlying cause (pain, anxiety, retained urine, constipation) without antihypertensive medications.
Hypotension
Hypotension is a sign, not a diagnosis. Always assess volume status, cardiac function, and perfusion.
Immediate Actions
- Recheck BP (verify it's not a cuff artifact)
- Review medications (timing, doses—did a vasodilator just get given?)
- Assess symptoms: Dizziness, chest pain, dyspnea, confusion
- Check telemetry: Arrhythmia? Bradycardia?
- Baseline BP: Is this patient's normal BP?
Clinical Assessment
- Exam: Skin perfusion, mental status, urine output, JVD, lung sounds, lower extremity edema
- Bedside ultrasound: IVC diameter and collapsibility (assess volume status); look for free fluid (bleeding) or pericardial effusion (tamponade)
Shock Classification

Stabilization
If hemodynamically unstable (altered mental status, signs of poor perfusion):
- Lay patient flat
- Activate rapid response/call attending
- Establish IV access (two large-bore lines)
- Begin fluid resuscitation (bolus 500mL–1L over 15–30min if hypovolemic)
- Supplemental oxygen to maintain SpO2 >94%
- Prepare for transfer to ICU
Diagnostic Labs and Imaging
| Test | Rationale |
|---|---|
| CBC | Evaluate for anemia, infection |
| Metabolic panel | Assess renal function, electrolytes, glucose |
| PT/INR | Coagulopathy assessment |
| Lactate | Marker of tissue hypoperfusion |
| Blood cultures | If sepsis suspected |
| Type & screen | For potential transfusion |
| EKG | Assess for ischemia, arrhythmia |
| CXR | Pulmonary edema, cardiomegaly, pneumonia |
| Transthoracic echo | Cardiac function, pericardial effusion, tamponade |
| CT PE protocol | If PE suspected (high risk, D-dimer positive) |
| Abdominal imaging | If occult bleeding suspected (CT with contrast) |
Ongoing Management
- Reassess BP and perfusion q15–30min until stable
- Avoid unnecessary diuretics (worsens hypovolemia)
- Target urine output ≥0.5mL/kg/h
- Persistent hypotension despite fluids: ICU transfer, central line placement, vasopressor consideration
Red Flag: Persistent Shock
If SBP remains <90 despite fluids, or if patient shows signs of end-organ dysfunction (creatinine rising, altered mental status), transfer to ICU immediately.
Confusion and Agitation
Confusion and agitation are NEVER nuisance calls. They represent acute changes in mental status that demand rapid evaluation for life-threatening causes.
Differential Diagnosis
Common etiologies in hospitalized patients:
- Medications: Anticholinergics, corticosteroids, dopamine agonists, antibiotics (fluoroquinolones, macrolides)
- Neurological: Stroke, intracranial hemorrhage, seizures
- Hypoxia/Hypercarbia: Low SpO2, high CO2 from respiratory failure
- Metabolic: Hypoglycemia, hyponatremia, hypercalcemia, uremia
- Infectious: Sepsis, UTI, meningitis, encephalitis
- Circulatory: Poor cerebral perfusion, arrhythmia
- Toxidromes: Anticholinergic, cholinergic, withdrawal (alcohol, benzodiazepines)
- Environmental: Dehydration, constipation, retained catheter/foley
Initial Assessment
- Vital signs: Fever (infection), tachycardia (sepsis, hypoxia), hypotension (shock)
- Recent medication administration: Timing and agents
- Physical violence risk: Assess for danger to self/others before approaching
- Catheter/lines: Retained foley, feeding tube (common delirium triggers)
Diagnostic Workup (Order Immediately)
| Test | Rationale |
|---|---|
| Accucheck | Hypoglycemia is reversible; check first |
| Pulse oximetry/ABG | Hypoxia, hypercarbia |
| CBC with differential | Infection, anemia |
| Metabolic panel | Na, glucose, Cr, urea |
| Urinalysis | UTI (often subtle in elderly) |
| Urine and blood cultures | Infection workup |
| EKG | Arrhythmia, ischemia |
| CXR | Pneumonia, pulmonary edema |
| Head CT | If focal deficits, trauma, or sudden onset |
| Urine drug screen | Assess for intoxication, withdrawal |
Specific Interventions by Cause
| Cause | Immediate Action |
|---|---|
| Hypoglycemia | Dextrose 50% 1 amp IV or IM glucagon |
| Opioid overdose | Naloxone 0.4mg IV |
| Benzodiazepine overdose | Flumazenil 0.2mg IV (caution: seizure risk) |
| Stroke concern | STAT head CT; call neurology |
| Seizure | Lorazepam 2–4mg IV; EEG if persistent seizure |
| Withdrawal (CIWA score) | Benzodiazepine dosing per CIWA protocol |
| Sepsis | Blood cultures, broad-spectrum antibiotics, fluids |
| Hypercarbia | Assess ventilation; consider intubation if severe |
Pharmacologic Management
Only after reversible causes are addressed.
Oral Medications (for agitation with some cooperation)
| Drug | Dosing | Notes |
|---|---|---|
| Quetiapine | 12.5–25mg PO | Start low; minimal orthostasis at low doses |
| Haloperidol | 2–5mg PO (1mg if elderly) | Typical antipsychotic; monitor QTc |
| Risperidone | 0.5–1mg PO | Atypical; less dystonia risk |
| Olanzapine | 2.5–5mg PO | Atypical; lower dystonia risk |
| Aripiprazole | 2–5mg PO | Atypical; use if QTc >500ms |
IM/IV Medications (for severe agitation, no cooperation)
| Drug | Dosing | Duration | Notes |
|---|---|---|---|
| Haloperidol | 2–5mg IV/IM | 4–6 hours | Monitor QTc; max 20mg/day |
| Olanzapine | 2.5–5mg IM | 4–6 hours | Good IM option |
| Ziprasidone | 10mg IM | 2–4 hours | Lower dystonia; good short-term use |
Nonpharmacologic Strategies
- Reorientation: Frequent interaction, clock/calendar visible, family presence
- Environmental: Minimize stimuli (dim unnecessary lights, reduce alarm volume)
- Comfort: Address pain, ensure adequate bathroom access
- Lines/tubes: Remove unnecessary catheters, central lines, feeding tubes
- Monitoring: 1:1 sitter for safety; bed alarm for fall risk
- Avoid restraints unless absolutely last resort (increase agitation, thromboembolism risk)
QTc Monitoring
Obtain EKG before and periodically during antipsychotic therapy. Discontinue if QTc >500ms.
Avoid Benzodiazepines and Anticholinergics
These worsen delirium. Reserve benzodiazepines only for seizure, severe withdrawal, or acute anxiety in specific contexts. Never use anticholinergics (diphenhydramine, scopolamine).
Fall Evaluation and Prevention
Falls cause significant morbidity. Systematic evaluation is essential.
Circumstances of Fall
- Witnessed vs. unwitnessed: Affects diagnostic approach
- Syncope: Loss of consciousness suggests arrhythmia, severe hypotension
- Weakness: Stroke, spinal cord compression, severe infection
- Incoordination: Cerebellar process, intoxication, medication toxicity
- Confusion: Delirium, hypoglycemia
- Environmental: Unsafe mobility aids, bed height, obstacles
Medication Review
- Excessive sedation from recent doses (opioids, sedatives, anticholinergics)
- Antihypertensives causing orthostasis
- Over-aggressive diuresis
- Recent initiation of drugs affecting balance
Physical Examination
- General: Height of fall, landing surface, immediate complaints
- Head/neck: Trauma, lacerations, palpable step-offs
- Neuro exam: Mental status, focal deficits, cranial nerves, strength
- Orthostatics: BP and HR lying/sitting/standing
- ROM: Painful areas, restricted movement suggesting occult fracture
- Skin: Lacerations, contusions, integrity
Diagnostic Imaging
| Indication for CT Head/Spine | Indication for X-rays |
|---|---|
| Fall from height on anticoagulants | Complaints of pain in specific area |
| Loss of consciousness | Mechanism suggests fracture |
| Focal neurological deficit | Immobility/inability to bear weight |
| High-risk mechanism | Fall in elderly on anticoagulation |
Fall Prevention Orders
- Bed alarm: Alert staff if patient attempts to exit bed
- Fall precautions sign: Visual alert for all staff
- 1:1 sitter: If high fall risk (delirium, intoxication, recent fall)
- PT/OT evaluation: Mobility assessment, safe walking aids
- Medication review: Consider holding sedating agents if possible
- Environmental: Bedside commode, clear pathways, adequate lighting
Constipation
Constipation is uncomfortable and can precipitate delirium. Assess for obstruction before treating.
Red Flags for Obstruction
Before prescribing laxatives, exclude bowel obstruction:
- Severe abdominal pain or distension
- Absence of flatus or stool for >48h
- Persistent nausea/vomiting
- Abdominal tenderness or guarding
- Consider abdominal X-ray (AXR) if obstruction suspected
Laxatives in Obstruction
Administering laxatives in the setting of mechanical obstruction can cause perforation. Always assess for obstruction first.
Medication Review
Discontinue or reduce if possible:
- Opioids (primary culprit; nearly all patients on opioids require bowel regimen)
- Anticholinergics (diphenhydramine, atropine, scopolamine patches)
- Antihistamines (first-generation H1 blockers)
Bowel Regimen Strategy
Start all patients on opioids with a scheduled bowel regimen from day one. Progress through medications as needed.
| Agent | Dosing | Onset | Mechanism | Notes |
|---|---|---|---|---|
| Docusate | 100mg PO BID | 24–72h | Stool softener | Ineffective as monotherapy |
| Miralax | 17g PO daily–BID | 1–4 days | Osmotic (polyethylene glycol) | Safe, well-tolerated |
| Magnesium hydroxide | 30–60mL PO | 6–12h | Osmotic | Avoid in renal failure; rapid onset |
| Magnesium citrate | 150mL PO | Rapid (1–2h) | Osmotic | Very rapid; use when urgent |
| Lactulose | 10–30cc PO q4–6h | 1–2h | Osmotic (galactose) | Causes bloating; less tolerated |
| Senna | 2–4 tablets PO daily–BID | 6–12h | Stimulant | Natural alternative |
| Bisacodyl | 10–30mg PO or PR | 6–10h | Stimulant | Rectal suppository faster |
| GoLytely | 4L PO or NG tube | 1–2h | Osmotic (polyethylene glycol solution) | Very aggressive; reserved for severe impaction |
Refractory Opioid-Induced Constipation
- Methylnaltrexone (Relistor): 8mg or 12mg SC every other day; peripheral mu-opioid antagonist (doesn't cross BBB, so preserves analgesia)
- Rectal interventions: Glycerin suppositories, bisacodyl suppositories, enemas (avoid Fleet in renal failure—risk of hyperphosphatemia)
- Manual disimpaction: Last resort; may require sedation and GI consultation
Proactive Bowel Management
Do not wait for constipation to develop. Initiate bowel regimens proactively when starting opioids, anticholinergics, or high-dose iron.
Diarrhea
Diarrhea can rapidly lead to dehydration and electrolyte derangement.
Etiologic Assessment
- Infectious: C. difficile (recent antibiotics, hospitalization), viral, bacterial (Salmonella, Shigella)
- Medication-induced: Antibiotics, magnesium-based laxatives, proton pump inhibitors, metformin
- Dietary: High sorbitol, lactose intolerance
- Inflammatory: IBD
- Functional: Irritable bowel syndrome
Clinical Evaluation
- Frequency, volume, consistency: Small frequent stools vs. large volume?
- Blood/mucus: Suggests infectious or inflammatory process
- Abdominal pain, fever: Infection vs. medication effect
- Recent antibiotic use: C. difficile concern
- Hydration status: Orthostasis, urine output, mucous membranes
Symptomatic Treatment
| Drug | Dosing | Notes |
|---|---|---|
| Loperamide | 4mg initial dose, then 2mg after each loose stool | Maximum 16mg/day; avoid in bloody diarrhea or toxic megacolon |
| Bismuth subsalicylate | 30mL PO q6h | Anti-inflammatory; acceptable for most infectious diarrhea |
Avoid Antidiarrheals in
- Bloody diarrhea (risk of toxic megacolon)
- Suspected C. difficile (can worsen toxin-mediated injury)
- High fever or severe abdominal pain
Fluid Replacement
- IV fluids if unable to tolerate PO or severe losses
- Electrolyte replacement (especially potassium if on diuretics)
- Consider stool studies/C. difficile testing if persistent or blood-stained
Seizure and Status Epilepticus
Seizures represent acute brain dysfunction. Rapid recognition and treatment are essential.
Definitions
- Seizure: Single event of abnormal electrical discharge
- Status epilepticus: Continuous seizure activity lasting >5 minutes OR recurrent seizures without recovery of consciousness between events
Immediate Actions (ABCS)
- Airway: Position on side, avoid forced objects in mouth
- Breathing: Ensure adequate ventilation; consider oxygen
- Circulation: Establish IV access, continuous monitoring
- Seizure termination: See medication algorithm below
Identify Reversible Causes
Treat underlying etiology:
- Hypoglycemia: Dextrose 50% 1 amp IV (or 25g glucose PO if conscious)
- Hyponatremia: Sodium replacement
- Hypocalcemia: Calcium gluconate
- Hypomagnesemia: Magnesium replacement
- Opioid toxicity: Naloxone 0.4–0.8mg IV
- Alcohol/sedative withdrawal: Benzodiazepines
- Infection/sepsis: Antibiotics after cultures
- Intracranial pathology: Head CT after seizure control
Diagnostic Labs and Imaging
| Test | Rationale |
|---|---|
| Glucose | Hypoglycemia common cause |
| Electrolytes (Na, Ca, Mg) | Imbalance can trigger seizures |
| ABG | Assess oxygenation, acidosis |
| Anticonvulsant levels | If known epileptic on medications |
| Toxicology screen | Withdrawal, intoxication |
| CBC | Infection, anemia |
| Blood cultures | If infection suspected |
| Head CT | Rule out hemorrhage, structural lesion |
| EEG | Continuous monitoring if altered mental status or recurrent seizures |
Medication Protocol for Seizure Termination

First-Line (Benzodiazepines)
Choose one:
- Lorazepam: 0.1mg/kg IV push (typical dose 4mg IV over 2 min); can repeat x2 at 5-min intervals
- Midazolam: 0.15mg/kg IV or IM (typical dose 10mg); repeat x2 if needed (onset slightly faster than lorazepam IM)
Second-Line (if first-line fails after 3–5 minutes)
Choose one:
- Levetiracetam: 60mg/kg IV (max 4500mg); infuse over 15 min
- Fosphenytoin: 20mg phenytoin equivalents (PE)/kg IV (safer than phenytoin); infuse at ≤150mg PE/min
- Valproic acid: 30mg/kg IV; infuse at ≤6mg/kg/min
- Phenytoin: 20mg/kg IV slow push; monitor cardiac rhythm (risk of arrhythmia, hypotension)
Refractory Status Epilepticus
If seizure persists despite 2 rounds of first-line and second-line agents:
- Intubate (protect airway, enable sedation)
- Continuous infusions (maintain seizure suppression for 24h after last clinical seizure):
- Midazolam: 0.1–2mg/kg/h IV
- Propofol: 1–3mg/kg/h IV (risk of propofol infusion syndrome with prolonged use)
- Phenobarbital: 15–40mg/kg loading, then 0.5–2mg/kg/h maintenance
- Transfer to ICU with neuromonitoring and EEG capability
Post-Seizure Management
- Continue second-line antiepileptic for 24h after last seizure before tapering
- Head imaging (CT or MRI) to exclude structural lesion
- EEG if status lasted >30min or multiple recurrences
- Neurology consultation
- Assess for aspiration risk; consider NPO pending evaluation
Timing is Critical
Status epilepticus causes permanent neurological injury and death. Aim to terminate seizures within 3–5 minutes of onset.
Shortness of Breath
Dyspnea is a common emergency. Rapid assessment of etiology guides management.
Differential Diagnosis

Initial Rapid Assessment
Immediately determine:
- Severity: Can complete sentences? Sitting upright? Cyanotic? Altered mental status?
- Vital signs: RR, HR, BP, SpO2, temperature
- Timeline: Acute (minutes), subacute (hours), chronic (days)
- Last known O2 requirement: Baseline oxygenation status?
- Code status: Resuscitation preferences?
Physical Examination
| Finding | Differential |
|---|---|
| Tachypnea (RR >30) | Pulmonary edema, pneumonia, PE, metabolic acidosis |
| Accessory muscle use | Obstructive airway disease, severe hypoxia |
| Cyanosis | Severe hypoxemia |
| Wheezing | Asthma, COPD, CHF (cardiac asthma) |
| Crackles | Pneumonia, pulmonary edema, atelectasis |
| Decreased breath sounds | Pneumothorax, pleural effusion, severe airflow obstruction |
| JVD | Right-sided heart failure, tamponade, tension pneumothorax |
| Lower extremity edema | Right heart failure, DVT/PE |
| Reproducible chest wall pain | Musculoskeletal; less likely to be serious |
Diagnostic Workup
| Test | Rationale |
|---|---|
| ABG | Assess oxygenation, CO2, acid–base status |
| CXR | Pneumonia, pneumothorax, pulmonary edema, cardiomegaly |
| EKG | Ischemia, arrhythmia, signs of PE |
| Troponin | ACS assessment |
| D-dimer/CT PE protocol | PE evaluation (especially if risk factors present) |
| Echocardiogram | Ventricular function, pericardial effusion, RV strain |
| CBC | Anemia, infection |
| Procalcitonin | Infection likelihood (if not already on antibiotics) |
Oxygen Therapy Escalation
Apply oxygen to maintain SpO2 >94% (>90% in COPD with hypercarbia risk).
| Modality | FiO2 Delivered | Use |
|---|---|---|
| Nasal cannula | 24–40% | Mild hypoxemia, comfort |
| Face mask | 40–60% | Moderate hypoxemia |
| Venturi mask | 24–50% (precise) | COPD with hypercarbia concern |
| Non-rebreather mask (NRB) | 60–95% | Severe hypoxemia; use as bridge |
| High-flow nasal cannula (HFNC) | Up to 100% | Severe hypoxemia, post-extubation support |
| BiPAP | Variable (titrate FiO2) | Hypercapnic respiratory failure, pulmonary edema |
BiPAP Settings for Respiratory Support
| Setting | Starting Value | Titration |
|---|---|---|
| IPAP (inspiratory) | 10 cmH2O | Increase if poor oxygenation/ventilation |
| EPAP (expiratory) | 5 cmH2O | Increase if refractory hypoxemia |
| FiO2 | 100% (titrate down) | Reduce as oxygenation improves |
Criteria for ICU/Intubation
Consider transfer to ICU or intubation if:
- SpO2 <90% despite 50–100% NRB oxygen
- Respiratory rate >35 or <8
- Severe accessory muscle use, diaphoresis, altered mental status
- Inability to protect airway or handle secretions
- PaO2 <60mmHg or PaCO2 >50mmHg on ABG
- pH <7.3 (respiratory acidosis)
- No improvement on BiPAP after 1–2h
Respiratory Failure
Respiratory failure is defined as pO2 <60 or pCO2 >50 with pH <7.3. Do not delay intubation if hemodynamically unstable or rapidly deteriorating.
Hypoglycemia
Symptomatic hypoglycemia (glucose <70 mg/dL) requires immediate treatment.
Risk Assessment Before Treatment
- How low is the glucose? (affects urgency)
- Diabetic vs. non-diabetic patient? (influences treatment)
- First episode or recurrent? (recurrent suggests medication issue)
- Insulin regimen or sulfonylureas? (higher hypoglycemia risk)
- NPO status? (affects feeding strategy)
- Renal/hepatic failure? (affects glucose metabolism)
- Adrenal insufficiency? (contributes to recurrent hypoglycemia)
Symptomatic vs. Asymptomatic
- Symptomatic: Tremor, diaphoresis, anxiety, palpitations, altered mental status → treat immediately
- Asymptomatic: Incidental low glucose check → cautious treatment to avoid over-correction
Acute Treatment
If symptomatic:
| Route | Dose | Onset | Notes |
|---|---|---|---|
| IV dextrose 50% | 1 amp (50mL = 25g glucose) | Immediate | Preferred if unable to take PO |
| IM/SC glucagon | 1mg | 10–15 min | Effective even if altered mental status; teaches family self-injection |
| PO dextrose | 15g carbs (4oz juice, 4 glucose tablets) | 10–15 min | Only if awake and cooperating |
Follow-up Glucose Checks and Treatment Adjustments
| Glucose Range | Action |
|---|---|
| <70 mg/dL and symptomatic | Treat with IV dextrose or glucagon; repeat check in 15 min |
| 70–100 mg/dL | Give PO carbs (10–15g) plus protein; recheck in 1h |
| >100 mg/dL after treatment | Resume normal diet; sign out to day team |
Ongoing Management Based on Diabetes Status
Patients WITHOUT diabetes
- PO option: Juice, glucose tablets, crackers with peanut butter; recheck in 15 min
- No insulin: Do not initiate unless diabetes diagnosed
Patients WITH diabetes
- Hold glucose-lowering agents (insulin, sulfonylureas, metformin)
- PO option: 15g fast-acting carbs (juice); recheck in 15 min
- No PO option: D50 IV or glucagon 1mg IM; repeat checks until glucose >100
- Persistent/recurrent hypoglycemia: Continuous IV dextrose infusion
Continuous Dextrose Infusions
Use for persistent hypoglycemia refractory to bolus dosing.
| Infusion | Indication |
|---|---|
| D5W or D5½NS at 75–150mL/h | Standard approach; adequate for most patients |
| D10 at 50–100mL/h | Use in ESRD/CKD or CHF (fluid-restricted patients) |
| D20 or D25 | Requires central line (risk of phlebitis); rarely used |
Medication Adjustments
- Sulfonylureas/meglitinides: Hold until glucose normalized; reassess dosing
- Insulin: Reduce dose or hold until glucose trend improves
- Other agents (metformin, GLP-1 agonists): Hold during hypoglycemia phase; restart once stable
Avoid Over-Treatment
Overcorrection to glucose >200 is common and worsens outcomes. Use 15g carbs, wait 15 min, and recheck. Do not give repeat doses of IV dextrose without rechecking glucose.
Hyperglycemia
Hyperglycemia in hospitalized patients is common. Determine if acute management or sign-out is appropriate.
Assessment
- Glucose trend over 24h: Single elevated check vs. persistent elevation?
- Symptoms: Polyuria, polydipsia, DKA/HHS warning signs (Kussmaul respirations, fruity breath, altered mental status)?
- Recent medications: D5/D10 fluids, corticosteroids, vasopressors?
- Baseline glucose control: Diabetic already, or new hyperglycemia?
Inpatient Target Glucose
- General ward: 140–180 mg/dL acceptable (tighter control increases hypoglycemia risk)
- ICU: 140–180 mg/dL (avoid <110, risk of neuroglycopenia)
- Perioperative: 180 mg/dL upper limit
Asymptomatic Mild-to-Moderate Hyperglycemia (140–300 mg/dL)
- Sliding scale insulin: Short-acting insulin based on glucose level
- Sign out to day team: Allow their endocrinology/diabetes management
- Monitor glucose: q6h initially, then q4h if trending up
Symptomatic or Severe Hyperglycemia (>300 mg/dL)
Suspect DKA or HHS if:
- Glucose >300–400
- Symptomatic: Polyuria, polydipsia, altered mental status, Kussmaul respirations
- Metabolic derangement: Check BMP for anion gap metabolic acidosis
- Ketones: Urine ketones or serum beta-hydroxybutyrate positive
If DKA/HHS suspected: - Call Endocrinology stat - Transfer to ICU (high-dose insulin infusion, aggressive fluid resuscitation) - Labs: BMP (anion gap, K, Cr), venous/arterial pH, serum beta-hydroxybutyrate, lactate - IV fluids: Normal saline at high rate (typically 500–1000mL/h initially) - Insulin infusion: 0.1 units/kg/h (typically 5–10 units/h)
Medication Review
- Remove D5/D10 fluids: Switch to D5W with insulin or non-dextrose-containing IV fluids
- Hold corticosteroids if possible or reduce dose
- Reduce vasopressor support if glucose normalizing
- Adjust renal replacement if on CRRT (dextrose-free dialysate if available)
Stacking Risk in Renal Failure
Avoid giving extra short-acting insulin doses in patients with rising creatinine or ESRD (risk of stacking and prolonged hyperinsulinemia). Use longer-acting agents or insulin infusion instead.
Day Team Sign-Out
Most modest hyperglycemia (140–250) can be safely signed out with a note to recheck glucose and adjust insulin regimen. Reserve ICU transfer for DKA/HHS or glucose >500 with symptoms.
Fever (Temperature ≥100.4°F/38°C)
Fever is a sign of infection or other serious illness. Systematic evaluation is essential.
Initial Assessment
- First fever or persistent? (first suggests new infection; persistent suggests inadequate treatment or resistant organism)
- Existing source of infection? (known pneumonia, UTI, surgical site—is it worsening?)
- Recent antibiotics started? (adequate coverage for anticipated organisms?)
- Chronic indwelling lines? (central line, foley—risk of device-associated infection)
- Immunosuppression? (steroids, malignancy, HIV—atypical presentations expected)
Common Fever Sources in Hospitalized Patients
| Source | Risk Factors | Red Flags |
|---|---|---|
| Pneumonia (PNA) | Intubation, aspiration, immobility | Cough, sputum, hypoxia, infiltrate on CXR |
| Urinary tract infection (UTI) | Foley catheter, female | Dysuria, frequency, pyuria on UA |
| Osteomyelitis | Recent surgery, prosthetic joints | Localized bone/joint pain, swelling |
| Intra-abdominal pathology | Recent surgery, perforated viscus | Abdominal pain, guarding, sepsis |
| Cellulitis | IV lines, skin breakdown | Erythema, warmth, edema at site |
| Clostridioides difficile (C. diff) | Recent antibiotics | Diarrhea (often bloodless), abdominal pain |
| Sacral pressure ulcers | Immobility, poor nutrition | Stage III/IV ulcers, purulent drainage |
| Surgical site infection | Post-op day 3–7 | Erythema, drainage, dehiscence |
Non-Infectious Causes of Fever
- Thromboembolism: DVT, PE (fever often low-grade, may lag symptoms)
- Atelectasis: Post-op or immobile patients
- Aspiration: Food, gastric contents → aspiration pneumonia
- Drug-induced: Antibiotics (beta-lactams), anticonvulsants
- Transfusion reaction: Within hours of product infusion
- Uremia: Elevated urea in end-stage renal disease
- Malignancy: Tumor burden itself
- Neuroleptic malignant syndrome: Recent antipsychotic; accompanied by rigidity, high CK
- Malignant hyperthermia: Perioperative; life-threatening
- Thyroid storm: Thyrotoxicosis; tachycardia, altered mental status
- Alcohol/benzodiazepine withdrawal: Autonomic hyperactivity
Diagnostic Workup
| Test | Rationale |
|---|---|
| Blood cultures x2 | Before antibiotics; aerobic and anaerobic bottles |
| Urinalysis and urine culture | UTI assessment |
| CBC with differential | WBC elevation, bands suggest bacterial infection |
| Comprehensive metabolic panel | Assess renal function, glucose, electrolytes |
| PT/INR, PTT | Assess for DIC (severe sepsis) |
| Lactate | Marker of tissue hypoperfusion; prognostic |
| CXR | Pneumonia, atelectasis, pulmonary edema |
| Procalcitonin (if not already on antibiotics) | Higher sensitivity/specificity for bacterial infection |
| CT abdomen/pelvis | If abdominal pain, post-op, perforation concern |
| Lower extremity ultrasound | DVT assessment if immobile |
| Stool studies | C. difficile toxin if diarrhea present |
| Lumbar puncture | Meningitis concern (fever + headache + neck stiffness + altered mental status) |
Empiric Antibiotic Coverage
If sepsis suspected (fever + hemodynamic instability, lactate elevated, altered mental status):
- Start broad-spectrum antibiotics immediately after blood cultures
- Common empiric regimen: Ceftriaxone or cefepime + vancomycin (add gentamicin if Pseudomonas risk)
- Consider local antibiogram and patient risk factors for resistant organisms
If source identified:
- PNA: Ceftriaxone ± azithromycin (community-acquired); Cefepime/Pip-tazo (hospital-acquired)
- UTI: Ceftriaxone or fluoroquinolone (if uncomplicated); cefepime if pyelonephritis/sepsis
- Cellulitis: Cefazolin or cephalexin; vancomycin if MRSA concern
- C. difficile: Vancomycin 125mg PO q6h (IV ineffective—poor colonic penetration)
Symptom Management
For fever ≥103°F:
- Acetaminophen: 650mg PO/PR; do not exceed 4g/day
- Ibuprofen: 400mg PO q6h (if no contraindications)
- Cooling measures: Cooling blankets, tepid sponging if very high fever (>104°F)
Fever as Defense Mechanism
Fever is the body's immune response (HEAT trial showed no benefit to aggressive fever reduction). Treat discomfort, but do not aggressively lower fever unless approaching critical temperature (>104°F) or in specific populations (cardiac disease, elderly).
Inadequate Initial Coverage
Do not delay antibiotics while awaiting culture results. Start empiric coverage immediately if sepsis suspected. De-escalate once sensitivities available.
Atrial Fibrillation with Rapid Ventricular Response (RVR)
Atrial fibrillation is common in hospitalized patients. Distinguish rate-controlled AF from RVR requiring acute intervention.
Initial Assessment
- New vs. known AF? (new AF requires urgent workup)
- Rate: Is HR >120 or >100 at rest? (defines RVR)
- Hemodynamically stable? (SBP >90, no chest pain, no acute pulmonary edema)
- Symptoms: Palpitations, chest pain, dyspnea, syncope?
- Last known rhythm: EKG and prior records?
Precipitants (Often Reversible)
| Trigger | Mechanism |
|---|---|
| Missed home beta-blocker/CCB | Loss of rate control |
| Excessive caffeine | Stimulant effect |
| Acute coronary syndrome | Ischemia triggers arrhythmia |
| Acute heart failure | Elevated atrial pressure |
| Pulmonary embolism | Acute RV strain |
| Hypoxia | Low SpO2 from any cause |
| COPD/asthma exacerbation | Airway inflammation |
| Thyrotoxicosis | Excess thyroid hormone |
| Hypokalemia | Low serum K |
| Hypomagnesemia | Low serum Mg |
| Alcohol/withdrawal | Autonomic destabilization |
| Sepsis | Systemic inflammation |
| Pain, anxiety, fever | Sympathetic stimulation |
Diagnostic Workup for New AF
| Test | Purpose |
|---|---|
| 12-lead EKG | Confirm AF, assess rate, look for ischemia |
| CBC | Infection, anemia |
| Metabolic panel | K, Mg, Cr, glucose |
| Troponin | ACS assessment |
| TSH | Thyroid dysfunction |
| CXR | Cardiomegaly, pulmonary pathology |
| Echocardiogram | Ventricular function, structural heart disease (if new AF) |
| D-dimer/CT PE | PE assessment if risk factors |
Rate Control Strategy
Hemodynamically STABLE AF-RVR
Goal: HR <110 at rest (lenient rate control per RATE-AF trial shows safety)
First-line agents:
| Drug | Dosing | Mechanism | Cautions |
|---|---|---|---|
| Metoprolol | 5–10mg IV q4–6h | Beta-blocker | Avoid if hypotensive or bradycardic; caution in asthma/COPD |
| Diltiazem | 10mg IV bolus; repeat at 15mg if needed; may start drip at 5–10mg/h | Calcium channel blocker | Avoid if hypotensive, bradycardic, or in acute CHF |
| Verapamil | 2.5–5mg IV slow push | Calcium channel blocker | Caution: negative inotrope |
If inadequate response:
- Amiodarone: 150mg IV bolus over 10 min, then 360mg infusion over 6h, then 540mg over 18h (rate control + rhythm control)
- Esmolol: Ultra-short-acting beta-blocker; 50–300mcg/kg/min IV drip (useful if need rapid titration/reversal)
- Digoxin: 0.5–1mg loading (slower onset; useful in CHF; narrow therapeutic window)
Hemodynamically UNSTABLE AF-RVR
If SBP <90, pulmonary edema, chest pain, or altered mental status:
- Lower-dose rate control: Reduced doses of metoprolol (2.5–5mg) or diltiazem (5mg), assess response
- Avoid aggressive dosing (risk of cardiogenic shock)
- Consider alternatives:
- Amiodarone: Maintains better hemodynamic stability
- Esmolol: Rapid titration and reversal
- Digoxin: In CHF (improves contractility while slowing AV node)
Severely Unstable AF-RVR
If the patient looks like they're dying (SBP <80, altered mental status, severe pulmonary edema, ongoing chest pain):
- Synchronized electrical cardioversion: 100–200J biphasic (sedate first if conscious)
- Prepare: ICU, intubation capability, defibrillator at bedside
Rhythm Control vs. Rate Control
- Lenient rate control (target HR <110): Safe for most patients with AF-RVR
- Rhythm control (convert to sinus rhythm): Consider if new AF, hemodynamic instability, or symptoms persist despite rate control
- Antiarrhythmic agents (flecainide, sotalol): Requires cardiology consultation; more risks in structural heart disease
Most AF in Hospital
Most AF-RVR in hospitalized patients is secondary to a reversible cause (pain, anxiety, fever, medication non-compliance). Address the precipitant; rate control often resolves as the underlying issue improves.
Stroke Risk in New AF
New-onset AF carries stroke risk. Discuss anticoagulation (apixaban, rivaroxaban, dabigatran, edoxaban) with attending or cardiology. Do not delay anticoagulation in absence of contraindication.
Chest Pain
Chest pain is a medical emergency until proven otherwise. Rapid evaluation is essential.
Immediate Triage
If any of these present → Call EMS, establish IV, continuous telemetry, oxygen, EKG immediately:
- Severe pressure/tightness
- Diaphoresis, pallor
- Hemodynamic instability
- Respiratory distress
Characterization
Obtain rapid history:
- Onset: Sudden vs. gradual? What were you doing?
- Quality: Pressure, sharp, pleuritic, burning, tearing?
- Radiation: Neck, arm, jaw, back?
- Associated symptoms: Dyspnea, nausea, diaphoresis, palpitations?
- Cardiac risk factors: Age, smoking, diabetes, hypertension, family history, prior MI/stent?
- Medication history: Cocaine, stimulants?
Physical Examination
| Finding | Significance |
|---|---|
| Reproducibility with palpation | Suggests musculoskeletal (but doesn't rule out ACS) |
| Asymmetric blood pressures (>20mmHg diff) | Aortic dissection concern |
| Unequal breath sounds or hyperresonance | Pneumothorax |
| New murmur | Acute valve disease (endocarditis, dissection) |
| Absent pulses in extremity | Dissection, thromboembolism |
| Unilateral leg swelling/warmth | DVT → PE risk |
| Rub on auscultation | Pericarditis |
| Hypotension, JVD, muffled heart sounds | Tamponade (Beck's triad) |
Life-Threatening Diagnoses to Rule Out
| Condition | EKG Finding | Imaging | Action |
|---|---|---|---|
| Acute MI (STEMI) | ST elevation | Troponin positive | Cardiology stat; cath <90 min |
| Acute MI (NSTEMI/UA) | ST depression, T-wave changes | Troponin positive | Antiplatelet, anticoagulation, cardiology consult |
| Aortic dissection | Usually normal | CTA chest (gold standard) | Cardiothoracic surgery stat; BP control |
| Pulmonary embolism | Sinus tachycardia (nonspecific) | CT angiography | Anticoagulation (if low bleeding risk) |
| Pneumothorax | Sinus tachycardia | CXR, CT if unclear | Chest tube if large/tension |
| Esophageal rupture | Nonspecific | CT with oral contrast | Surgery stat (high mortality) |
| Acute pericarditis | Diffuse ST elevation, PR depression | Echocardiogram | NSAIDs, colchicine; serial ECGs |
| Tension pneumothorax | Extreme tachycardia (dying) | Clinical diagnosis | Needle decompression followed by chest tube |
Rapid Diagnostic Workup
| Test | Timing |
|---|---|
| EKG | Within 10 min of arrival |
| Troponin (high-sensitivity) | Stat; repeat at 3h if initial negative and concern remains |
| CXR | Within 15 min |
| CBC, CMP | Baseline labs |
| D-dimer or CT angiography | If PE suspected |
| Echocardiogram | If pericarditis, tamponade, or valvular disease suspected |
| CT chest with contrast | If aortic dissection concern |
ACS Management (STEMI/NSTEMI/Unstable Angina)
STEMI: - Call cardiology stat: Percutaneous coronary intervention (PCI) target door-to-balloon <90 minutes - ASA: 325mg (unless allergy) - Anticoagulation: Unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) - Nitroglycerin: 0.3–0.6mg SL; repeat q5min if SBP >90; hold if RV infarction (right-sided EKG leads) or hypotensive
NSTEMI/Unstable Angina: - Cardiology consultation (may not need emergent cath; can risk-stratify) - Dual antiplatelet therapy: ASA 325mg + loading dose of P2Y12 inhibitor (clopidogrel 600mg, prasugrel 60mg, or ticagrelor 180mg) - Anticoagulation: UFH or LMWH - Beta-blocker: Metoprolol or carvedilol (if stable BP and HR) - Statin: High-intensity statin (atorvastatin 80mg or rosuvastatin 40mg) - NTG: As above for symptom relief - Morphine: 2–4mg IV for pain not relieved by NTG; repeat q5–15min
Aortic Dissection
Suspect with tearing chest/back pain, especially if hypertensive or Marfan syndrome. Blood pressure control is critical (target SBP 100–120 and HR 60); use beta-blocker first, then vasodilator. Do NOT delay CTA imaging.
EKG Leads Matter
Always obtain right-sided leads (V3R, V4R) if inferior MI suspected (RV involvement). RV infarction is preload-dependent; avoid aggressive nitroglycerin/diuretics (can cause cardiogenic shock).
Acute Anemia
Acute anemia (falling hemoglobin/hematocrit) requires rapid evaluation and stabilization.
Risk Stratification
Determine urgency:
- Hemoglobin level: >10 usually tolerates without transfusion; <7 often requires transfusion
- Hemodynamic stability: Hypotension or tachycardia indicates hemodynamic compensation
- Bleeding source: Known vs. occult bleeding
- Cardiac history: ACS, CHF—lower tolerance for anemia
Etiologic Assessment
| Source | Risk Factors | Red Flags |
|---|---|---|
| GI bleeding | PUD, varices, anticoagulants | Hematemesis, melena, hematochezia |
| Surgical site bleeding | Recent surgery, anticoagulation | Drainage, expanding hematoma, fluctuant swelling |
| Concealed bleeding | Trauma, coagulopathy, anticoagulation | Abdominal pain, flank ecchymosis, retroperitoneal hemorrhage |
| Hemolysis | G6PD, autoimmune, prosthetic valve | Elevated bilirubin, LDH, jaundice, dark urine |
| Nutritional deficiency | Chronic bleeding, poor diet | Macrocytic (B12/folate), microcytic (iron) anemia |
| Bone marrow failure | Chemotherapy, myelodysplasia, sepsis | Pancytopenia (low WBC, Plt) |
Clinical Evaluation
| Finding | Differential |
|---|---|
| Hemodynamic instability | Active major bleeding; transfuse immediately |
| Orthostatic vital signs | Volume depletion; IV fluids and transfusion |
| Melena or bright red blood per rectum | GI source |
| Abdominal pain, guarding | Retroperitoneal bleed, perforation |
| Jaundice, dark urine, palpable spleen | Hemolysis |
| Petechiae, bleeding gums | Thrombocytopenia, coagulopathy |
Diagnostic Labs
| Test | Purpose |
|---|---|
| CBC with differential | Confirm anemia; assess WBC, platelets (pancytopenia suggests bone marrow issue) |
| Reticulocyte count | Bone marrow response to bleeding (elevated in hemolysis/acute bleeding) |
| Coagulation studies (PT/INR, PTT) | Assess for coagulopathy |
| Fibrinogen, D-dimer | DIC assessment |
| Type & screen or crossmatch | Blood product availability |
| Peripheral blood smear | Hemolysis (schistocytes), infections, malignancy |
| Comprehensive metabolic panel | Renal function, K, glucose |
| Bilirubin, LDH, haptoglobin | Hemolysis workup |
| Reticulocyte hemoglobin | Assesses iron stores (low in iron deficiency) |
| Rectal exam with FOBT | GI source assessment |
Transfusion Strategy
| Hemoglobin | Clinical Context | Action |
|---|---|---|
| <7 g/dL | Any patient | Transfuse 1 unit pRBC; recheck Hgb; goal Hgb 7–9 |
| 7–10 g/dL | Stable, no bleeding | Consider transfusion if symptoms (dyspnea, chest pain) or ongoing bleeding |
| 7–8 g/dL | ACS/cardiac history | Transfuse to Hgb 8–9 (lower tolerance for anemia) |
| >10 g/dL | No active bleeding | Treat underlying cause; transfuse only if continued bleeding |
Management of Ongoing Bleeding
If bleeding continues despite transfusion:
- Maintain two large-bore IVs (consider central line if difficult access)
- Type & cross additional units (prepare for massive transfusion protocol)
- Activate massive transfusion protocol if anticipated need for >4 units PRBC in 24h
- Obtain imaging (CT angiography if pulmonary source; abdominal CT if intra-abdominal source)
- Consult GI, surgery, interventional radiology as indicated
- Hold anticoagulation (unless life-threatening indication like PE/ACS)
- Correct coagulopathy (FFP, platelets, cryoprecipitate as needed)
Avoid Over-Transfusion
Transfusion carries risks (fluid overload, TRALI, infection). Use restrictive strategy (transfuse at Hgb <7) except in specific populations (ACS, symptomatic anemia).
Patient Requesting to Leave AMA (Against Medical Advice)
Patients have the right to refuse treatment. However, certain patients cannot legally leave AMA.
Determination of Capacity
Before accepting an AMA request, the patient must have decision-making capacity:
- Understands their medical condition
- Understands the proposed treatment
- Understands the consequences of refusal
- Can communicate their choice consistently
Patients WITHOUT capacity cannot leave AMA: - Advanced dementia with no surrogate decision-maker - Acute delirium with inability to reason - Intoxicated or actively withdrawing from substances - Involuntary psychiatric hold (1013 hold)
Attempt to Retain Patient
- Understand the reason: Why do they want to leave? (Pain, cost, misconception, family emergency?)
- Address concerns: Can you solve the underlying problem?
- Involve case management and social work for resource barriers (financial, transportation, housing)
- Involve family (if appropriate) in discussion
- Clearly explain risks: What could happen if they leave without complete treatment?
AMA Documentation
If patient insists on leaving after discussion:
- Contact the attending physician immediately (do not allow departure without attending knowledge)
- Have patient sign AMA form (document understanding of risks)
- Document in chart:
- Statement of patient's reason for leaving
- Medical risks explained (be specific)
- Capacity assessment and findings
- Plan for follow-up (outpatient appointment, primary care referral)
- Patient's understanding of treatment alternatives
- Witness signature (RN, MD, or both)
- Provide discharge instructions (medications, follow-up appointments, warning signs)
Involuntary Psychiatric Hold (1013)
Patients on psychiatric hold cannot legally leave the hospital. Requires psychiatry clearance before release. Do not discharge against 1013 hold without attending psychiatry approval.
Pronouncing a Death
Pronouncing death is a somber but essential skill. Always perform a thorough examination.
Confirmation of Death
Examine for signs of death:
| Finding | Timeline |
|---|---|
| Absent pulse (check brachial/carotid for 60 sec) | Immediate |
| No heart sounds on auscultation | Immediate |
| Absent breathing (listen for breath sounds; no fog on mirror) | Immediate |
| Fixed, dilated pupils (nonreactive to light) | Within minutes |
| Pallor mortis (paleness of skin) | Within 15 min |
| Rigor mortis (body stiffening) | 2–6 hours |
| Livor mortis (dependent purple discoloration) | 20–30 min |
| Algor mortis (cooling of body) | Hours |
Pronounced Exam
In the presence of family (if appropriate):
- Auscultate heart (listen >60 seconds)
- Auscultate lungs
- Palpate pulse (carotid and brachial)
- Assess pupil reactivity to light
- Note absence of breath sounds/movement
- Check for any response to painful stimuli
Time of death = time you complete the examination (not time of last vital signs or last observed movement)
Death Certificate and Documentation
- Death note in medical record:
- Time of examination
- Vital signs findings (all absent)
- Physical exam findings
- Time death pronounced
- Circumstances (expected vs. sudden)
-
Attending physician name
-
Death certificate (legal requirement):
- Must be completed by attending physician
- Primary cause of death + contributing conditions
- Submit to vital records within specified timeframe
-
Family responsible for funeral home arrangements
-
Notify family (if not present):
- Compassionate but direct communication
- Offer support services (chaplaincy, social work, grief counseling)
-
Explain what happens next (organ donation discussion, funeral home contact)
-
Release of body:
- To funeral home of family's choice
- Requires signed release form
- No autopsy unless requested/indicated
Family Presence
When possible, allow family to be present during examination and at time of death pronouncement. Provides closure and validates the loss. Offer continued support and grief resources.
Summary: Key Pearls for Night Call
- Assess before treating: Every symptom has a differential. Rule out serious causes before giving comfort medications.
- Recheck vitals: Many "urgent" issues resolve after rechecking BP, SpO2, or blood glucose.
- Call early: Don't wait to escalate; transfer to ICU sooner rather than later for unstable patients.
- Know your limits: When unsure, involve the senior resident or attending early.
- Document thoroughly: Your note may be the only record of overnight events.
- Communicate handoffs: Clearly sign out to the day team; don't leave surprises.
- Sleep when you can: Fatigue impairs judgment; prioritize your safety and your patients' safety.
Laboratory Abnormalities
This guide provides evidence-based approaches to diagnosing and managing common laboratory derangements encountered in internal medicine practice.
Electrolyte Replacement Protocols
Potassium Repletion
Potassium supplementation depends on the serum level and patient factors. Always consider renal function before aggressively replacing.
| Serum K+ (mEq/L) | Oral Replacement | IV Replacement | Frequency |
|---|---|---|---|
| 3.6-3.8 | 40 mEq | 20 mEq | Once |
| 3.3-3.5 | 40 mEq | 20 mEq | Every 2-4 hours, twice total |
| 2.8-3.2 | 40 mEq | 20 mEq | Every 2-4 hours, three times total |
| <2.8 | 40 mEq | 20 mEq | Every 2-4 hours, three times + additional IV support |
Caution in Renal Disease
Patients with end-stage renal disease, chronic kidney disease, or acute kidney injury have impaired urinary potassium excretion. Use significantly less aggressive replacement strategies to avoid hyperkalemia. Consider nephrology consultation if K+ <2.8 in these populations.
Clinical Pearls - Potassium
- Approximately 10 mEq of potassium raises serum concentration by 0.1 mEq/L
- Oral and intravenous replacement have equivalent efficacy
- Magnesium depletion causes increased urinary potassium wasting—always check and correct magnesium concurrently
- Recheck serum levels approximately 2 hours after completing supplementation
- Low magnesium levels (<1.6 mEq/L) perpetuate hypokalemia and should be repleted first
Magnesium Repletion
Magnesium supplementation is essential when levels fall below normal, as hypomagnesemia impairs the kidney's ability to retain potassium.
| Serum Mg (mg/dL) | IV MgSO4 Dose | Infusion Duration | Notes |
|---|---|---|---|
| 1.8-2.0 | 1 g | 2 hours | Gradual replacement |
| 1.6-1.7 | 2 g | 2 hours | Moderate depletion |
| <1.5 | 2 g | 2 hours | Severe depletion; may require repeat dosing |
Magnesium Replacement Calculation
Each 1 gram of magnesium sulfate administered intravenously raises serum magnesium concentration by approximately 0.1 mg/dL. Monitor and recheck levels after completing infusion.
Phosphorus Repletion
Phosphate supplementation addresses severe hypophosphatemia. Choose the salt based on concurrent sodium and potassium status.
| Serum PO4 (mg/dL) | Sodium Phosphate Dose | Infusion Duration | Clinical Approach |
|---|---|---|---|
| 2.0-2.4 | 15 mmol | 4 hours | Mild depletion; slower infusion acceptable |
| 1.0-1.9 | 30 mmol | 4 hours | Moderate depletion |
| <1.0 | 45 mmol | 4 hours | Severe depletion; monitor closely |
Potassium Phosphate Considerations
- Use potassium phosphate for oral replacement when serum phosphate is >2 mg/dL or if sodium is elevated
- Each mmol of potassium phosphate contains 1.5 mEq of potassium—account for this when calculating total daily potassium load
- Monitor serum sodium and potassium carefully when using potassium phosphate preparations
Hyponatremia (Serum Sodium <135 mEq/L)
Hyponatremia results from excess total body water relative to sodium. The workup follows a systematic approach: establish true hyponatremia, determine volume status, and identify the underlying cause.
Initial Workup
Begin by measuring three key parameters:
- Serum osmolality (measured or calculated)
- Urine osmolality
- Urine sodium concentration
Normal reference values: Urine sodium ~20 mEq/L, Urine osmolality 50-1200 mOsm/kg, Serum osmolality 280-303 mOsm/kg
Step 1: Confirm True Hyponatremia
Calculate serum osmolality using the formula:
Serum Osmolality = 2×(Na + K) + (Glucose ÷ 18) + (BUN ÷ 2.8)
Compare calculated osmolality to the measured value to classify the hyponatremia:
Hypertonic (Pseudohyponatremia)
Measured osmolality > Calculated osmolality
Occurs when the serum contains unmeasured osmotically active particles. Serum sodium appears low but tonicity is normal.
- Hyperglycemia: Each 100 mg/dL of glucose above 100 requires correction using: Corrected Na = Measured Na × 1.6
- Toxic ingestions: Methanol, ethylene glycol, propofol
- Hypertriglyceridemia or hyperproteinemia: Laboratory artifact from laboratory analysis technique
Isotonic (Pseudohyponatremia)
Measured osmolality ≈ Calculated osmolality
Serum osmolality is normal despite low reported sodium value. This is a laboratory error from elevated lipids or proteins that displace the aqueous phase.
Hypotonic (True Hyponatremia)
Measured osmolality < Calculated osmolality
Genuine hyponatremia with decreased serum tonicity. This is the form requiring treatment. Proceed with volume status assessment.
Step 2: Assess Volume Status
Determine intravascular volume by clinical examination and laboratory findings:

Hypovolemic Hyponatremia
Laboratory findings: Urine sodium <20 mEq/L OR Fractional excretion of sodium <1%
Extrarenal causes: Gastrointestinal losses (vomiting, diarrhea, nasogastric drainage), hemorrhage, reduced oral intake, third-space sequestration
Renal causes: Diuretic use, nephropathies, primary adrenal insufficiency, secondary adrenal disease, cerebral salt-wasting syndrome
Treatment: Address the underlying cause, restore intravascular volume - Mild cases: Oral rehydration with sodium-containing beverages (sports drinks) if tolerated - Moderate to severe: Normal saline 0.9% intravenously, titrated to clinical response - Adjust rate based on symptomatic improvement and sodium correction
Euvolemic Hyponatremia
Diagnostic approach: Urine osmolality patterns distinguish the cause
SIADH (Syndrome of Inappropriate ADH Secretion)
- Urine osmolality >100 mOsm/kg (inappropriately concentrated)
- Urine sodium >40 mEq/L
- Euvolemic on clinical exam
- Serum osmolality low despite concentrated urine
Common causes: - Malignancy: Small-cell lung cancer, pancreatic cancer, gastric cancer, genitourinary cancers, lymphomas - Pulmonary disorders: Pneumonia, tuberculosis, chronic obstructive pulmonary disease - Intracranial pathology: Head trauma, subarachnoid hemorrhage, ischemic stroke, seizures - Medications: Antipsychotics, selective serotonin reuptake inhibitors, chemotherapy agents, NSAIDs
Treatment: Free water restriction to <1000 mL daily; address underlying cause; consider vaptans for severe cases
Psychogenic Polydipsia
- Urine osmolality <100 mOsm/kg (dilute)
- Typically requires daily fluid intake >12 liters
- Often associated with psychiatric disease
- Treatment: Patient education, fluid restriction, psychiatric support
Low Solute Intake
- Dilute urine (osmolality <100)
- Low urine sodium (<20 mEq/L)
- History of unusual diet patterns
- Examples: "Tea and toast" diet in elderly, beer potomania (excessive beer consumption with minimal food)
- Treatment: Nutritional counseling, increase sodium and protein intake
Hypervolemic Hyponatremia
Laboratory findings: Edema present clinically; urine sodium varies by cause
CHF (Congestive Heart Failure)
- Urine sodium <10 mEq/L
- Fractional excretion of sodium <1%
- Mechanism: Decreased cardiac output stimulates renin-angiotensin-aldosterone system and ADH secretion
- Pathophysiology: Renal arterial hypotension and hepatic congestion perpetuate sodium retention
Cirrhosis
- Severe hepatic dysfunction with portal hypertension
- Splanchnic arterial vasodilation leads to systemic hypotension perception
- Compensatory activation of RAAS and ADH
- Often associated with ascites
Nephrotic Syndrome
- Severe hypoalbuminemia from proteinuria
- Oncotic pressure reduction allows fluid translocation to interstitium
- Compensatory RAAS and ADH activation
- Sodium retention and volume expansion despite clinical appearance of depletion
Advanced Renal Failure
- Urine sodium >20 mEq/L
- Fractional excretion of sodium >1%
- Severely reduced glomerular filtration rate impairs water and sodium excretion
Treatment: Loop diuretics (furosemide), fluid restriction, sodium restriction; address underlying cardiac or hepatic disease
Severity Classification
| Severity | Sodium Level | Clinical Features |
|---|---|---|
| Mild | 130-134 mEq/L | Often asymptomatic |
| Moderate | 120-129 mEq/L | Nausea, headache, confusion |
| Severe | <120 mEq/L | Seizures, coma, cerebral edema, death |
Acuity: Distinguishing Acute vs. Chronic
- Acute onset (<48 hours): Brain has not had time to adapt; lower osmolar threshold before symptoms develop
- Chronic onset (>48 hours): Cerebral adaptation through loss of intracellular osmolytes protects against cerebral edema
Clinical significance: Chronic hyponatremia tolerance allows lower sodium levels before symptoms; acute hyponatremia at higher levels (125-130) can cause severe neurologic symptoms
Treatment Strategy
General Principles
- Identify and treat the underlying etiology
- Discontinue contributory medications (SSRIs, antipsychotics, NSAIDs, diuretics)
- Restrict free water intake appropriately for the volume status
- Monitor closely during correction to avoid overcorrection
Specific Approaches by Volume Status
Hypovolemic: - Mild cases: Sodium-containing beverages if tolerated - Moderate/severe: Normal saline 0.9% intravenously
Euvolemic: - SIADH: Free water restriction <1000 mL daily - Low solute: Nutritional counseling, increase sodium/protein intake
Hypervolemic: - Fluid restriction (goal <1000 mL daily) - Loop diuretics (furosemide) at high doses for volume reduction
Severe/Acute Hyponatremia (Na <110 mEq/L or symptomatic with seizure/coma)
Hyponatremic Crisis Management
- Administer 3% hypertonic saline 100 mL intravenous bolus
- May repeat bolus up to two additional times if seizures persist
- Goal is to raise sodium rapidly enough to stop cerebral edema and seizure activity
- Then transition to slower correction
Correction Rate and ODS Prevention
Risk of Osmotic Demyelination Syndrome
Overly rapid sodium correction causes osmotic demyelination syndrome (ODS), characterized by myelinolysis in the pons and extrapontine regions, leading to permanent neurologic disability.
Correction limits: - Never exceed 1 mEq/L per hour - Goal: 0.25-0.5 mEq/L per hour - Maximum daily correction: 6-8 mEq/L in first 24 hours (conservative approach unless acute symptomatic) - Unless severe/acute crisis: Correct 4-6 mEq/L in <6 hours total
High-risk patients for ODS: - Severe hyponatremia (Na <105) - Concurrent hypokalemia - Alcoholic liver disease - Malnutrition - Advanced liver disease
Preventing Overcorrection
- Monitor serum sodium every 1 hour during moderate/severe cases
- After initial stabilization, check every 2-6 hours
- Consider administering desmopressin 2 mcg intravenously every 6-8 hours to limit aquaresis if at risk for overcorrection
- Prevents continued free water loss from osmotic diuresis
Intravenous Fluid Sodium Content
When choosing intravenous fluids, consider the sodium concentration:
| Fluid Type | Sodium Content (mEq/L) | Use |
|---|---|---|
| Lactated Ringer (LR) | 130 | Maintenance, mild hyponatremia |
| Normal Saline (NS, 0.9%) | 154 | Hypovolemic hyponatremia |
| 3% Hypertonic Saline | 513 | Severe/symptomatic hyponatremia |
| 1/2 NS (0.45%) | 77 | Caution in hyponatremia; provides free water |
Fluid Selection Pearls
- Do not use D5W (dextrose 5% in water) in isolation for hyponatremia; high glucose becomes osmotically active
- Do not use D5 1/2NS as it provides free water and worsens hyponatremia
- LR and NS may actually increase serum sodium concentration if patient is significantly volume depleted, but their sodium concentrations are lower than serum so they provide relative free water at higher concentrations
- Consider the underlying cause when selecting fluid (CHF needs fluid restriction, not more saline)
Hypernatremia (Serum Sodium >145 mEq/L)
Hypernatremia represents a water deficit relative to sodium stores. The pathophysiology centers on insufficient free water intake, excessive free water loss, or sodium overload. Always think of this as a water problem, not a sodium problem.
Etiology and Urine Osmolality Classification
Measure urine osmolality to determine if the kidneys are responding appropriately to hypernatremia:
Extrarenal (Renal Appropriately Concentrating)
Urine osmolality >700-800 mOsm/kg
The kidneys are concentrating urine maximally in response to hypernatremia, indicating appropriate ADH function.
- Gastrointestinal losses: Diarrhea, small bowel fistulas, ileostomy
- Insensible losses: Fever, sweating from exercise, mechanical ventilation, burns
Renal (Kidneys Cannot Concentrate Adequately)
Urine osmolality <700-800 mOsm/kg
The kidneys fail to concentrate urine despite hypernatremia, indicating ADH insufficiency or nephrogenic resistance.
- Osmotic diuresis: Hyperglycemia, mannitol administration, contrast exposure
- Loop diuretic therapy: Furosemide, torsemide
- Diabetes insipidus (Central): Hypothalamic/pituitary dysfunction from trauma, surgery, granulomatous disease, malignancy
- Diabetes insipidus (Nephrogenic): Kidney resistance to ADH from lithium, demeclocycline, hypercalcemia, hypokalemia
Other Mechanisms
- Sodium overload: Normal saline administration, hypertonic saline, sodium bicarbonate
- Impaired thirst mechanism: Elderly, altered mental status, unable to access water
- Seizures or extreme exertion
Initial Workup
- Check urine osmolality to guide diagnostic approach
- Assess urine sodium
- Evaluate volume status clinically (may be masked by hyperosmolality)
- Review medications and recent procedures
Treatment Approach
The goal is slow free water replacement to avoid cerebral edema from osmotic water influx into the brain.
Step 1: Volume Resuscitation
Begin by addressing severe volume depletion if present. Be cautious: normal saline (Na 154) and lactated Ringer (Na 130) may paradoxically increase serum sodium if the patient is very hypernatremic, because their sodium concentration is less than the patient's serum sodium.
Step 2: Calculate Free Water Deficit
Use available calculators (MDCalc) to estimate total body water deficit. Formula:
Free Water Deficit (L) = Current TBW × [(Serum Na - 145) / 145]
Where total body weight = weight (kg) × age-adjusted water fraction (0.5 for older women, 0.6 for older men, 0.7 for younger men)
Step 3: Replace Free Water Deficit
Choose replacement fluid based on severity and acuity:
| Fluid Choice | Sodium (mEq/L) | Use Case |
|---|---|---|
| Oral water | 0 | If safe to drink and GI intact |
| Nasogastric free water flush | 0 | If unable to drink but NG tube present |
| D5W (dextrose 5% water) | 0 (becomes free water after glucose metabolism) | IV if necessary |
| 1/2 NS (0.45% saline) | 77 | Slower correction in stable patients |
Fluids to Avoid
- Do NOT use normal saline (0.9%) in hypernatremia unless severe volume depletion requiring aggressive resuscitation
- Do NOT use 3% saline unless there is concurrent hyponatremia or life-threatening hypernatremia
- Do NOT use full NS or more concentrated solutions for deficit replacement
Step 4: Monitor and Adjust
- Check serum sodium and basic metabolic panel every 4 hours initially
- Transition to twice-daily monitoring once stable
- Goal correction rate: 2 mEq/L per 4-hour assessment interval
- Never exceed 0.5 mEq/L per hour to avoid cerebral edema
- Adjust infusion rate based on response
Specific Treatment Considerations
For Osmotic Diuresis: Treat the underlying hyperglycemia or discontinue osmotic agents; this will reduce urine output and allow serum sodium to normalize more slowly
For Central Diabetes Insipidus: Replace free water deficit; may add desmopressin (synthetic ADH) if unable to replace orally
For Nephrogenic Diabetes Insipidus: Free water replacement is the mainstay; consider thiazide diuretics (which paradoxically reduce urine output in nephrogenic DI), NSAIDs, and adequate hydration
Hypokalemia (Serum Potassium <3.5 mEq/L)
Hypokalemia indicates total body potassium depletion or shift of potassium intracellularly. Even modest decreases can cause significant cardiac and muscle dysfunction.
Etiologies
Classify by mechanism and measure urine potassium (UK) and transtubular potassium gradient (TTKG) to guide diagnosis:
Transcellular Shift (UK <25 mEq/L, TTKG <3)
Potassium moves into cells; serum depletion without total body deficit
- Metabolic alkalemia: Stimulates cellular uptake
- Insulin administration: Drives potassium intracellularly
- Catecholamine excess: Beta-2 agonists, high-dose epinephrine
- Hypothermia: Shifts potassium intracellularly
- Antipsychotic overdose: Clozapine causes hypokalemia through unclear mechanism
Gastrointestinal Losses (UK <25 mEq/L, TTKG <3)
Total body potassium depleted through GI tract without renal compensation
- Diarrhea: Most common cause of hypokalemia
- Laxative abuse
- Vomiting and nasogastric suction: Indirect effect through acid loss and metabolic alkalosis
- Small bowel or pancreatic fistulas
Renal Losses (UK >30 mEq/L, TTKG >7)
Kidneys unable to retain potassium despite low serum levels
Normal-to-Low Blood Pressure + Acidosis: - Diabetic ketoacidosis (despite total body depletion, serum K appears normal initially) - Renal tubular acidosis (Types 1 and 2) - Chronic diuretic use - Hypomagnesemia (most common cause of refractory hypokalemia) - Bartter syndrome (inherited; mimics chronic diuretic effect) - Gitelman syndrome (inherited; similar to Bartter but milder)
Hypertension + Hypokalemia (Mineralocorticoid Excess): - Primary hyperaldosteronism (Conn syndrome): Adrenal adenoma or bilateral hyperplasia - Secondary hyperaldosteronism: Renal artery stenosis, malignant hypertension, diuretic use - Cushing syndrome: Excessive glucocorticoid effect on mineralocorticoid receptors - Liddle syndrome: Gain-of-function mutation in renal sodium channel - Licorice ingestion: Mineralocorticoid-like effect
Clinical Manifestations
| Severity | Symptoms | ECG Changes |
|---|---|---|
| Mild (3.0-3.5) | Often asymptomatic or vague | Minimal or absent |
| Moderate (2.5-3.0) | Muscle weakness, cramps, fatigue | Flattened T waves, prolonged QT |
| Severe (<2.5) | Paralysis, rhabdomyolysis, respiratory weakness | Prominent U waves, flattened T waves, prolonged PR interval |
Serious Complications
Severe hypokalemia can cause: - Ventricular fibrillation and sudden cardiac death - Myoglobinuria and acute kidney injury from rhabdomyolysis - Respiratory muscle paralysis - Cardiac arrhythmias, especially in patients on digoxin
Diagnostic Workup
- Spot urine potassium (UK) and urine sodium (UNa)
- Serum magnesium level (check in all cases)
- Basic metabolic panel (assess acid-base status)
- 12-lead ECG if K <2.6 or Mg <1.6
- Transtubular potassium gradient (TTKG) = (UK × Serum osmolality) / (Serum K × Urine osmolality)
- If renal losses: Blood pressure, plasma renin, aldosterone
Treatment
Always Treat Concurrent Hypomagnesemia
Magnesium depletion perpetuates hypokalemia and prevents successful potassium repletion. If serum magnesium <1.6 mEq/L, repleted concurrently using magnesium replacement protocol above.
Replacement Using Established Protocol
Follow the potassium replacement table presented in the Electrolyte Replacement Protocols section above.
Monitoring
- Check serum potassium 2 hours after completing oral replacement
- Recheck 2-4 hours after intravenous replacement
- Place on continuous cardiac monitoring if K <2.6 or Mg <1.6
Potassium Replacement Pearls
- Potassium chloride is the preferred formulation (other salts like phosphate or bicarbonate may cause other electrolyte abnormalities)
- Oral potassium causes GI upset; take with food or use extended-release formulations
- Expect 10 mEq replacement to raise serum K by 0.1 mEq/L (accounting for ongoing losses)
- Magnesium must be repleted to prevent recurrence
Hyperkalemia (Serum Potassium >5.5 mEq/L)
Hyperkalemia represents one of the most dangerous electrolyte disturbances, capable of causing sudden cardiac death. Severe cases require immediate recognition and rapid treatment.
Etiologies
Pseudohyperkalemia (In Vitro Artifact)
Elevated potassium is a laboratory finding without true systemic hyperkalemia:
- Hemolysis: Red blood cell rupture during blood draw or processing
- Thrombocytosis: Potassium release from platelets during clotting (>700,000/μL)
- Leukocytosis: Potassium release from white blood cells during clotting (>100,000/μL)
- IV fluid contamination: Potassium-containing solution mixed into sample
- Post-splenectomy: Elevated platelet counts from lack of splenic destruction
Distinction: Check plasma potassium (heparin tube) vs serum (clot tube); in pseudohyperkalemia, plasma K is normal
Transcellular Shift (Movement Into Cells)
Total body potassium normal but serum levels elevated:
- Acidemia: H+ shifts into cells in exchange for K+ moving out
- Insulin deficiency: DKA or severe hyperglycemia
- Beta-blocker administration: Prevents normal cellular uptake
- Digoxin toxicity: Inhibits Na-K-ATPase pump
- Massive cellular release: Tumor lysis syndrome, rhabdomyolysis, hemolysis, crushing injuries
Renal Retention (Most Common True Hyperkalemia)
Kidneys unable to excrete potassium:
- Acute kidney injury
- Chronic kidney disease (especially stages 4-5)
- Primary adrenal insufficiency
- Medications:
- ACE inhibitors (block aldosterone)
- Angiotensin receptor blockers (block aldosterone)
- NSAIDs (reduce renal perfusion, impair aldosterone synthesis)
- Trimethoprim-sulfamethoxazole (blocks renal potassium secretion)
- Heparin (suppresses aldosterone)
- Potassium-sparing diuretics (spironolactone, amiloride)
Other Causes
- Increased dietary potassium in susceptible patients
- Potassium supplement overuse
- Salt substitutes containing potassium
Clinical Manifestations
Hyperkalemia can present with nonspecific symptoms or appear asymptomatic until sudden cardiac death occurs.
| Level | Symptoms | ECG Changes |
|---|---|---|
| 5.5-6.0 | Often asymptomatic | Peaked T waves (in precordial leads) |
| 6.0-7.0 | Weakness, paresthesias, palpitations | Peaked T waves, prolonged PR, widened QRS |
| >7.0 | Severe weakness, cardiac palpitations, respiratory distress | Peaked T waves, prolonged PR, widened QRS, merged S and T (sine wave pattern) |
ECG Progression and Cardiac Risk
ECG changes progress as potassium rises: 1. Peaked T waves: Most sensitive early sign 2. Prolonged PR interval: Conduction slowing 3. Widened QRS complex: Ventricular conduction delay 4. Merged S and T waves: "Sine wave" pattern indicating severe hyperkalemia 5. Eventual asystole or ventricular fibrillation: Terminal rhythm
Critical action: When ECG changes present, treat immediately regardless of exact serum level
Diagnostic Approach
Check ECG First
Before anything else: Obtain a 12-lead ECG to identify cardiac toxicity. Do not wait for confirmation; treat based on ECG findings if present.
After ECG:
- Serum potassium (repeat to confirm, rule out pseudohyperkalemia)
- Plasma potassium if pseudohyperkalemia suspected (heparin tube)
- Basic metabolic panel (assess renal function, glucose, acid-base status)
- Urine potassium, urine sodium, urine osmolality (assess renal excretion capacity)
- Venous blood gas (assess for acidemia)
- Complete blood count (evaluate for thrombocytosis or leukocytosis)
Treatment
Treatment intensity depends on severity, ECG findings, and renal function.

Immediate Therapy (For ECG Changes or K >7)
| Agent | Dose | Onset | Mechanism | Duration |
|---|---|---|---|---|
| Calcium Gluconate | 1-2 amps IV | <3 minutes | Stabilizes cardiac membrane | 30-60 min |
| Insulin + Dextrose | 10 U regular insulin IV + 1-2 amps D50 | 15-30 min | Shifts K intracellularly | 4-6 hours |
| Albuterol | 10-20 mg nebulized | 15-30 min | Beta-2 agonism shifts K intracellularly | 4-6 hours |
| Sodium Bicarbonate | 1-2 amps IV | 15-30 min | Shifts K intracellularly (if acidotic) | 4-6 hours |
Calcium Administration
- Give if K >7 or ANY ECG changes present (peaked T waves or beyond)
- Does not lower serum potassium; merely stabilizes cardiac membrane to prevent arrhythmia
- Can repeat after 5 minutes if ECG changes persist
- Onset is fastest of all hyperkalemia treatments
Shift Agents (Lower Serum Potassium 0.5-1.2 mEq/L)
Insulin + Dextrose: Most effective - Give 10 units regular insulin intravenously - Accompany with 1-2 ampules of dextrose 50% to prevent hypoglycemia - Recheck potassium in 15-30 minutes - Effect lasts 4-6 hours; may repeat if needed
Albuterol: Adjunctive therapy - 10-20 mg via nebulizer - Can combine with insulin for additive effect - Less effective in patients on chronic beta-blockers
Sodium Bicarbonate: If acidotic - 1-2 ampules IV push - Works synergistically with insulin - Essential in metabolic acidemia
Elimination Agents (Excrete Potassium from Body)
These agents remove potassium and provide definitive treatment.
Kayexalate (sodium polystyrene sulfonate): Cation exchange resin - Dose: 30-90 g orally or rectally - Onset: Several hours - Binds potassium in GI tract and removes in stool - May mix with sorbitol to promote bowel movement - Effect lasts days to weeks
Patiromer: Newer cation exchanger - Dose: 8.4-25.2 g orally daily - Onset: ~30 minutes - Well-tolerated; less GI distress than kayexalate - Particularly useful for chronic hyperkalemia management
Loop Diuretics (if not in acute kidney injury): - Furosemide ≥40 mg IV - Increases urine potassium excretion - Onset: 30 minutes - Most effective in patients with preserved renal function
Hemodialysis: For severe, refractory hyperkalemia - Most effective in setting of acute kidney injury or dialysis-requiring renal failure - Removes potassium directly - Reserved for life-threatening cases or when other measures fail
Hyperkalemia Treatment Approach
- Stabilize the heart with calcium (if ECG changes present)
- Shift potassium intracellularly with insulin/dextrose, albuterol, bicarbonate
- Eliminate potassium from body with kayexalate, patiromer, furosemide, or dialysis
- Address the underlying cause: Reduce potassium intake, discontinue ACE-I/ARB, treat acidemia
- Recheck potassium: Every 2-4 hours initially until stable
Hypocalcemia (Total Calcium <8.4 mg/dL or Ionized Calcium <1.10 mmol/L)
Hypocalcemia causes neuromuscular hyperexcitability and can progress to life-threatening cardiac arrhythmias and seizures.
Etiologies
Hypoalbuminemia (Ionized Calcium Usually Normal)
Reduced albumin carries most circulating calcium; total calcium falls but ionized fraction (physiologically active) remains normal. Correct total calcium before assuming true hypocalcemia.
Hypoparathyroidism
Inadequate parathyroid hormone production: - Autoimmune destruction - Surgical removal during thyroid/parathyroid surgery - DiGeorge syndrome (22q11 deletion)
Pseudohypoparathyroidism
End-organ resistance to PTH despite elevated PTH levels
Vitamin D Deficiency
Insufficient 25(OH)D decreases intestinal calcium absorption: - Dietary insufficiency - Limited sun exposure - Malabsorption (Crohn's disease, celiac disease) - Nephrotic syndrome (loss of vitamin D binding protein)
Chronic Kidney Disease and Renal Failure
- Decreased 1,25(OH)2D synthesis
- Phosphate retention and hyperphosphatemia
- Secondary hyperparathyroidism development
Acute Phosphate Elevation (Calcium Sequestration)
- Acute pancreatitis: Saponification of fat with calcium precipitation
- Tumor lysis syndrome: Massive phosphate release from dying cells
- Phosphate infusion or phosphate-containing enemas
Hungry Bone Syndrome
Post-parathyroidectomy calcium influx into skeleton as parathyroid effect abruptly ceases
Clinical Manifestations
| Severity | Symptoms | Signs |
|---|---|---|
| Mild | Perioral numbness, paresthesias | Subtle |
| Moderate | Muscle cramps, tetany, anxiety | Trousseau sign, Chvostek sign |
| Severe | Seizures, laryngospasm, cardiac arrhythmia | Loss of consciousness, airway compromise |
Clinical Signs
- Trousseau sign: Carpopedal spasm with blood pressure cuff inflation
- Chvostek sign: Facial muscle contraction with facial nerve percussion (less specific)
- Tetany: Involuntary muscle contractions
- Osteomalacia: Bone pain and muscle weakness from chronic vitamin D deficiency
Diagnostic Workup
- Total serum calcium and ionized calcium (if total <8.5)
- Serum albumin (correct total calcium for albumin; corrected Ca = measured + 0.8 × [4.0 − albumin])
- Comprehensive metabolic panel: Creatinine, phosphate, magnesium
- PTH level (elevated in secondary hyperparathyroidism; low in hypoparathyroidism)
- Vitamin D metabolites: 25(OH)D (storage form) and 1,25(OH)2D (active form)
- 12-lead ECG: Assess for QT prolongation
- Consider magnesium level: Hypomagnesemia impairs PTH response
Treatment
Correct Serum Calcium for Albumin
Corrected Calcium = Measured Calcium (mg/dL) + 0.8 × (4.0 − Serum Albumin [g/dL])
This step is essential before deciding on aggressiveness of replacement.
Mild Hypocalcemia (Corrected Calcium 7.5-8.4 mg/dL)
Oral supplementation: - Calcium carbonate 1-2 g daily (taken with meals for absorption) - Calcium citrate 1-2 g daily (absorbed independently of acid) - Combined with vitamin D2 (ergocalciferol) 1000-2000 IU daily or vitamin D3 (cholecalciferol) 1000-2000 IU daily
Treatment duration: Days to weeks; recheck serum calcium weekly
Severe Hypocalcemia (Corrected Calcium <7.5 mg/dL or Symptomatic)
Intravenous calcium gluconate (preferred over calcium chloride outside central lines): - Dose: 1-2 grams intravenously over 20 minutes - Prepare as: 10 mL of 10% solution (1 gram) per 50-100 mL normal saline - Can repeat infusion if symptoms persist or calcium remains critically low - Recheck serum calcium 2 hours after infusion
IV Calcium Administration
- Do NOT mix with phosphate (forms precipitate)
- Do NOT infuse rapidly (causes cardiac arrhythmias, hypotension)
- Consider central line if repeated infusions anticipated (calcium gluconate is caustic to peripheral veins)
- Dilute appropriately in normal saline
- Monitor ECG during administration
Magnesium Repletion
Always check and correct hypomagnesemia if present (serum Mg <1.6 mEq/L) using magnesium replacement protocol above. Hypomagnesemia impairs the PTH response and perpetuates hypocalcemia.
Address Underlying Cause
- Vitamin D deficiency: Vitamin D supplementation (dose depends on 25[OH]D level and renal function)
- Hypoparathyroidism: Calcium and vitamin D replacement
- Acute kidney injury: Phosphate binders, treat hyperphosphatemia
- Pancreatitis: Supportive care; usually self-limited
- Tumor lysis: Aggressive hydration, allopurinol or febuxostat
Hypercalcemia (Serum Calcium >10.5-11 mg/dL; Severe Crisis: 14-16 mg/dL)
Hypercalcemia is a medical emergency when severe, as it causes dehydration, nephrogenic diabetes insipidus, cardiac arrhythmias, and altered mental status.
Etiologies
Only two diagnoses account for >90% of hypercalcemia cases: primary hyperparathyroidism and malignancy.
Primary Hyperparathyroidism
PTH-secreting parathyroid adenoma, hyperplasia, or rarely carcinoma. Accounts for approximately 50% of hypercalcemia in ambulatory settings.
Malignancy-Related Hypercalcemia
- PTHrP secretion (squamous cell lung cancer, renal cell carcinoma, breast cancer, ovarian cancer): Most common mechanism in hospitalized patients
- Osteolytic metastases: Direct bone destruction (breast cancer, lymphoma)
- Calcitriol production by tumor: Lymphomas (Hodgkin and non-Hodgkin), tuberculosis, histoplasmosis
Vitamin D Excess
- Exogenous supplementation: Toxic megadoses
- Endogenous overproduction: Granulomatous diseases (sarcoidosis, tuberculosis, fungal infections), lymphomas
Increased Bone Turnover
- Hyperthyroidism
- Thyrotoxicosis
- Immobilization (especially in young, active individuals)
- Vitamin A toxicity
- Paget disease (if immobilized)
Medications
- Thiazide diuretics: Decrease urinary calcium excretion
- Lithium: Raises PTH set point
- Vitamin D intoxication: From supplements or granulomatous disease
Milk-Alkali Syndrome
Excessive calcium and alkali (calcium carbonate + sodium bicarbonate) causing hypercalcemia, metabolic alkalosis, and renal insufficiency
Clinical Manifestations
"Stones, bones, groans, and psychiatric overtones"
| System | Manifestations |
|---|---|
| Renal | Nephrogenic DI (polyuria, polydipsia), acute kidney injury, kidney stones |
| GI | Nausea, vomiting, constipation, anorexia, peptic ulcer disease |
| Neuro | Altered mental status, confusion, lethargy, coma, headache |
| Cardiac | Arrhythmias, hypertension, shortened QT interval |
| Musculoskeletal | Bone pain, osteoporosis with fractures |
| Metabolic | Dehydration, metabolic alkalosis |
Diagnostic Workup
PTH: The Most Important Initial Test
Always obtain serum PTH level early. This single test narrows the differential dramatically.
- Serum PTH (most important initial test)
- Ionized calcium (if total calcium abnormal)
- Basic metabolic panel: Assess creatinine, phosphate
- Complete blood count: Evaluate for lymphoma
- Chest X-ray: Evaluate for sarcoidosis or malignancy
- 12-lead ECG: Assess for shortened QT interval
- Vitamin D metabolites: 25(OH)D and 1,25(OH)2D if PTH suppressed
- PTHrP level if PTH low and malignancy suspected
Interpretation Framework
If PTH elevated (>65 pg/mL): - Primary hyperparathyroidism (most common) - Check 24-hour urine calcium to distinguish from familial hypocalciuric hypercalcemia (FHH) - FHH: Very low urinary calcium (<100 mg/24h) - Primary hyperparathyroidism: Normal to high urinary calcium
If PTH suppressed (low): - Measure PTHrP (PTH-related peptide) - If elevated: Malignancy with PTHrP secretion - Measure vitamin D metabolites - If 1,25(OH)2D elevated: Granulomatous disease or lymphoma producing calcitriol - If 25(OH)D elevated: Exogenous vitamin D toxicity - Evaluate for osteolytic metastases, vitamin A toxicity, thiazide use
Treatment Strategy
Treatment intensity correlates with severity and symptoms. Asymptomatic mild hypercalcemia may be monitored; severe symptomatic hypercalcemia requires aggressive management.
Mild Hypercalcemia (Corrected Calcium <12 mg/dL, Asymptomatic)
Conservative approach: - Avoid thiazide diuretics (worsen hypercalcemia) - Avoid lithium (raises PTH set point) - Restrict dietary calcium intake - Ensure adequate hydration - Address underlying cause (parathyroidectomy for primary hyperparathyroidism) - Monitor serum calcium every 3-6 months
Moderate Hypercalcemia (Calcium 12-14 mg/dL)
Aggressive hydration + pharmacologic treatment:
| Intervention | Dose/Details | Onset |
|---|---|---|
| IV Normal Saline | 200-300 mL/hour | Immediate |
| Furosemide | 20-40 mg IV every 4-6 hours (after volume repletion) | 30-60 min |
| Calcitonin | 4 U/kg IV or IM every 12 hours | 2-4 hours |
| Bisphosphonate | Zoledronic acid 4 mg IV over 15 minutes (or pamidronate 60-90 mg) | 3-5 days |
Mechanism: - IV saline: Restores intravascular volume, promotes renal calcium wasting - Furosemide: Loop diuretic prevents excessive fluid expansion; promotes calcium excretion - Calcitonin: Inhibits osteoclast-mediated bone resorption; rapid onset but tachyphylaxis develops - Bisphosphonate: Blocks osteoclast bone resorption; slower onset but longer duration
Severe Hypercalcemia (Calcium >14 mg/dL or Life-Threatening Symptoms)
All measures above plus:
| Treatment | Details |
|---|---|
| Aggressive IV hydration | Fluid challenge; place central line if needed |
| Calcitonin | As above; addresses acute crisis |
| Bisphosphonate | As above |
| Hemodialysis | Consider if:Renal failure present; Unable to tolerate large fluid volumes (CHF, renal disease) |
| Glucocorticoids | 40-60 mg prednisone daily if granulomatous disease or lymphoma (calcitriol overproduction) |
| Ketoconazole | For granulomatous disease with excessive calcitriol production (coccidioidomycosis, histoplasmosis) |
Severe Hypercalcemia Management
In life-threatening hypercalcemia: - Start IV saline immediately (rates of 300-500 mL/hour) - Add calcitonin and bisphosphonate simultaneously - Monitor urine output, serum calcium, renal function closely - Have hemodialysis capability available if renal failure present - Treat underlying malignancy or parathyroid disease
Acid-Base Disorders
Acid-base interpretation requires systematic evaluation of arterial (or venous) blood gas with clinical context. A structured approach prevents errors and guides appropriate treatment.
Normal Values and Basic Concepts
| Parameter | Normal Range | Interpretation |
|---|---|---|
| pH | 7.35-7.45 | Acidemia <7.35; Alkalemia >7.45 |
| pCO2 | 35-45 mmHg | Reflects respiratory component |
| HCO3- | 22-26 mEq/L | Reflects metabolic component |
Arterial vs Venous Blood Gas
- ABG (Arterial): More accurate for pCO2; gold standard for acid-base assessment
- VBG (Venous): Acceptable surrogate in many clinical settings
- Concordant values: pH (add ~0.04 to VBG pH to approximate ABG), HCO3-
- Non-concordant: pCO2 differs between ABG and VBG; ABG required if pCO2 critical
Systematic Interpretation Approach

Step-by-Step Interpretation
Step 1: Identify Acidemia or Alkalemia
Determine if pH is low (<7.35) or high (>7.45).
Step 2: Identify Primary Process
Look at the respiratory and metabolic components: - Metabolic acidosis: Low HCO3- with low pH - Metabolic alkalosis: High HCO3- with high pH - Respiratory acidosis: High pCO2 with low pH - Respiratory alkalosis: Low pCO2 with high pH
The parameter that matches the pH direction is the primary disorder.
Step 3: Check Respiratory Compensation
Determine if respiratory response is appropriate for the primary process.
For Metabolic Acidosis — Use Winter's Formula:
Expected pCO2 = (HCO3- × 1.5) + 8 ± 2
- Actual pCO2 > Expected: Concurrent respiratory acidosis
- Actual pCO2 < Expected: Concurrent respiratory alkalosis
- Actual pCO2 ≈ Expected: Appropriate respiratory response
For Metabolic Alkalosis — Expected pCO2 rises 6-7 mmHg per 10 mEq/L rise in HCO3-:
- If actual pCO2 lower than expected: Concurrent respiratory alkalosis
- If actual pCO2 higher than expected: Concurrent respiratory acidosis
For Respiratory Acidosis:
| Duration | Expected HCO3- Change Per 10 mmHg pCO2 Rise |
|---|---|
| Acute (<24 hours) | +1 mEq/L |
| Chronic (>24-48 hours) | +3-4 mEq/L |
For Respiratory Alkalosis:
| Duration | Expected HCO3- Change Per 10 mmHg pCO2 Drop |
|---|---|
| Acute (<24 hours) | -2 mEq/L |
| Chronic (>24-48 hours) | -4-5 mEq/L |
Step 4: Calculate Anion Gap (for Metabolic Acidosis)
Anion Gap = [Na+] − ([Cl−] + [HCO3−])
Normal anion gap = 12 ± 2 mEq/L (can vary by laboratory)
Elevated anion gap = >14 mEq/L
Step 5: Delta-Delta (for Anion Gap Metabolic Acidosis)
When anion gap metabolic acidosis is identified, calculate whether a concurrent non-anion gap metabolic acidosis or metabolic alkalosis exists.
ΔAG = Change in Anion Gap = Measured AG − 12 ΔHCO3- = Change in HCO3- = 24 − Measured HCO3- ΔΔ = ΔAG / ΔHCO3-
Interpretation: - ΔΔ <1: Concurrent non-AG metabolic acidosis (HCO3- dropping faster than AG rising) - ΔΔ 1-2: Pure AG metabolic acidosis (appropriate relationship) - ΔΔ >2: Concurrent metabolic alkalosis (HCO3- not dropping as much as AG rising)
Metabolic Acidosis
Metabolic acidosis results from either bicarbonate loss or hydrogen ion accumulation.
Anion Gap vs. Non-Anion Gap Classification
Anion Gap Metabolic Acidosis (AG >14)
The anion gap exists because unmeasured anions accumulate to balance sodium. Common mnemonic: MUDPILES
| Cause | Mechanism | Notes |
|---|---|---|
| Methanol | Toxic metabolite formic acid | Osmolar gap present; visual symptoms |
| Uremia | Retention of organic acids | Late in renal failure; AG usually <20 |
| DKA | Ketone accumulation | Glucose >250; check beta-hydroxybutyrate |
| Propylene glycol | Toxic metabolite | Often iatrogenic (medications, IV solutions) |
| Isoniazid | Toxic metabolite | Tuberculosis treatment |
| Lactic acidosis | Lactate accumulation | Type A (hypoxemia) or Type B (mitochondrial) |
| Ethylene glycol | Toxic metabolite oxalic acid | Antifreeze ingestion; calciums oxalate crystals in urine |
| Salicylates | Aspirin toxicity | Mixed respiratory alkalosis + metabolic acidosis |
Winter's Formula Interpretation
Always calculate expected pCO2 using Winter's formula for any AG metabolic acidosis: - If actual pCO2 > expected → Concurrent respiratory acidosis - If actual pCO2 < expected → Concurrent respiratory alkalosis (typical in early DKA, lactic acidosis, and salicylate toxicity)
Non-Anion Gap Metabolic Acidosis
The anion gap is normal, but HCO3- is low. Causes involve GI bicarbonate loss or renal hydrogen ion retention. Determine using Urine Anion Gap (UAG).
UAG = [UNa+] + [UK+] − [UCl−]
| Urine Anion Gap | Interpretation | Common Causes |
|---|---|---|
| UAG Positive (>0) | Kidney cannot acidify urine; distal acidification defect | RTA Type 1, RTA Type 4, Chronic kidney disease |
| UAG Negative (<-20) | Appropriate acid excretion; GI bicarbonate loss | Diarrhea (most common), small bowel fistulas, ileostomy |
Treatment
- Identify and treat the underlying cause (remove toxin, treat infection, control diabetes)
- In severe acidemia (pH <7.1), consider sodium bicarbonate 100-150 mEq IV over 1-2 hours for metabolic acidosis, especially if severe and refractory
- In DKA: Insulin and fluids (bicarbonate generally avoided unless pH <6.9)
- In lactic acidosis: Treat underlying shock, improve tissue perfusion
Respiratory Acidosis
Respiratory acidosis results from inadequate ventilation, causing carbon dioxide retention.
Acute vs. Chronic Distinction
The kidney's ability to retain bicarbonate determines compensation:
For every 10 mmHg rise in pCO2 above 40: - Acute respiratory acidosis (<24 hours): HCO3- rises by 1 mEq/L (minimal renal compensation) - Chronic respiratory acidosis (>24-48 hours): HCO3- rises by 3-4 mEq/L (metabolic compensation)
Etiologies
| Category | Examples |
|---|---|
| CNS Depression | Sedatives, opioids, anesthetics, head trauma, sleep apnea |
| Neuromuscular Disorder | Myasthenia gravis, Guillain-Barre syndrome, polymyositis, amyotrophic lateral sclerosis |
| Chest Wall Abnormality | Flail chest, rib fractures, restrictive lung disease, severe obesity |
| Upper Airway Obstruction | Epiglottitis, foreign body, laryngospasm |
| Lower Airway/Lung Disease | COPD exacerbation, asthma, pneumonia, pulmonary edema, pulmonary fibrosis |
| Air Trapping | COPD with auto-PEEP, asthma, emphysema |
Treatment
- Identify and treat underlying cause
- Improve ventilation: Non-invasive positive pressure (CPAP, BiPAP) or mechanical ventilation if needed
- Support oxygenation
- Address concurrent metabolic abnormalities
Respiratory Alkalosis
Respiratory alkalosis results from hyperventilation, causing excessive carbon dioxide elimination.
Acute vs. Chronic Distinction
For every 10 mmHg drop in pCO2 below 40: - Acute respiratory alkalosis (<24 hours): HCO3- drops by 2 mEq/L (minimal renal compensation) - Chronic respiratory alkalosis (>24-48 hours): HCO3- drops by 4-5 mEq/L (metabolic compensation through increased urinary bicarbonate wasting)
Etiologies
| Cause | Mechanism |
|---|---|
| Pain | Splinting from acute pain, rib fractures, abdominal trauma |
| Anxiety | Panic attacks, hyperventilation syndrome |
| Hypoxemia | Fever, infection, pulmonary embolism, pneumonia, high altitude |
| Drugs | Salicylates (aspirin), stimulants, amphetamines |
| Fever | Increased metabolic rate drives hyperventilation |
| Pregnancy | Progesterone-mediated stimulation of respiratory center |
| Sepsis | Cytokine-mediated hyperventilation as early sign |
| Intracranial Pathology | Head trauma, intracerebral hemorrhage, seizures |
| Mechanical Ventilation | Overly aggressive ventilator settings |
Treatment
- Address underlying cause (treat infection, manage pain, reassure anxious patient)
- For hyperventilation from anxiety: Breathing exercises, rebreather bag if severe
- Adjust mechanical ventilation if iatrogenic
- Avoid overcorrection (overly rapid increase in pCO2 causes metabolic acidosis paradoxically)
Metabolic Alkalosis
Metabolic alkalosis results from bicarbonate excess or hydrogen ion loss. Classification by responsiveness to saline helps guide treatment.
Saline-Responsive Alkalosis (Urine Chloride <20 mEq/L)
Kidneys will excrete bicarbonate if given normal saline, indicating volume depletion as primary driver.
Causes: - Vomiting and nasogastric suction: Direct loss of hydrogen and chloride; metabolic alkalosis - Diuretic use: Loop and thiazide diuretics cause volume depletion and trigger RAAS activation - GI losses of hydrochloric acid: Small bowel/pancreatic fistulas
Treatment: Normal saline 0.9% IV at rates sufficient to correct volume deficit; typically 250-500 mL/hour. Potassium replacement often necessary simultaneously.
Saline-Resistant Alkalosis (Urine Chloride >20 mEq/L)
Kidneys cannot excrete bicarbonate because RAAS is activated from other mechanisms. Further saline worsens alkalosis.
Hypertensive Variants (Blood Pressure Elevated)
Primary hyperaldosteronism (Conn syndrome): - Autonomous aldosterone secretion from adrenal adenoma or bilateral hyperplasia - Severe hypokalemia - Low plasma renin - Elevated plasma aldosterone - Treatment: Spironolactone (aldosterone antagonist) or amiloride (potassium-sparing diuretic)
Secondary hyperaldosteronism from hypertension: - Renal artery stenosis, malignant hypertension, uncontrolled hypertension - RAAS activation from perceived hypoperfusion - Treatment: Control blood pressure; add potassium-sparing diuretics or ACE inhibitors
Cushing syndrome: Excess glucocorticoid effects on mineralocorticoid receptors - Treatment: Treat underlying pituitary or adrenal disease
Normotensive Variants (Blood Pressure Normal)
Severe hypokalemia: - Hypokalemia perpetuates alkalosis through multiple mechanisms - Treatment: Potassium replacement using protocols above; may require high doses
Bartter and Gitelman syndromes: Inherited renal tubular disorders - Mimic chronic diuretic use - Severe hypokalemia and alkalosis - Treatment: NSAIDs, potassium-sparing diuretics, amiloride
Respiratory Compensation in Metabolic Alkalosis
Respiratory response is typically minimal in metabolic alkalosis (unlike metabolic acidosis where hyperventilation is prominent). The respiratory system poorly matches alkalosis because hypoxemia is less tolerable than mild hypercapnia.
Expected pCO2 elevation: Approximately 6-7 mmHg per 10 mEq/L rise in HCO3-.
Treatment Strategy
| Alkalosis Type | Primary Treatment |
|---|---|
| Saline-responsive | Normal saline IV (0.9%) + potassium chloride replacement |
| Saline-resistant, Hypertensive | Antihypertensive agents (ACE inhibitors, ARBs); Aldosterone antagonists if appropriate |
| Saline-resistant, Normotensive | Potassium replacement (often high-dose); NSAIDs; Potassium-sparing diuretics |
| Severe (pH >7.6) | Hydrochloric acid or acetazolamide in addition to above measures |
Summary: Quick Reference Table
| Abnormality | Key Diagnostic Finding | Initial Treatment | Critical Monitoring |
|---|---|---|---|
| Hypokalemia | K <3.5; TTKG <3 if renal cause | Replace per protocol; always check Mg | Recheck K in 2h; ECG if K <2.6 |
| Hyperkalemia | K >5.5; peaked T waves on ECG | Calcium (stabilize), insulin/dextrose (shift), kayexalate (eliminate) | ECG first; recheck K q2-4h |
| Hyponatremia | Na <135; measured osm < calculated | Identify cause; free water restriction ±saline | Correct slowly; avoid ODS; check Na q1-2h |
| Hypernatremia | Na >145; free water deficit | Calculate deficit; replace with free water | Correct slowly (0.25-0.5 mEq/L/hr); check Na q4h |
| Hypocalcemia | Ca <8.4; correct for albumin | IV calcium gluconate if severe; oral Ca + vitamin D | Recheck Ca 2h after IV; check Mg |
| Hypercalcemia | Ca >10.5; check PTH | IV saline + calcitonin ± bisphosphonate | Hourly Ca if >14; assess renal function |
| AG Metabolic Acidosis | HCO3- low; AG >14; Winter's formula | Treat underlying cause (DKA, lactic acidosis, toxins) | Follow pH, anion gap closure |
| Non-AG Metabolic Acidosis | HCO3- low; AG normal; UAG negative | Treat diarrhea; identify RTA type if UAG positive | Correct slowly with bicarbonate |
| Respiratory Acidosis | pH <7.35; pCO2 >45 | Improve ventilation; identify CNS/NM/airway cause | Serial ABGs; support ventilation |
| Respiratory Alkalosis | pH >7.45; pCO2 <35 | Treat underlying cause; avoid overcorrection | Follow pCO2 trend; prevent paradoxical acidosis |
| Metabolic Alkalosis | pH >7.45; HCO3- >26; UCl <20 (saline-responsive) | Normal saline + KCl; identify etiology | Check BP; correct K concurrently |
Clinical Pearls and Key Take-Homes
Always Remember
- Magnesium: Check in all hypokalemia and hypomagnesemia independently; repletion is essential for K correction success
- Volume status: Critical for guiding hyponatremia treatment; never give hypertonic saline to euvolemic patient
- ECG in hyperkalemia: Check it first, before waiting for lab confirmation; peaked T waves demand treatment
- Winter's formula: Use in every case of metabolic acidosis to identify concurrent respiratory disorders
- Anion gap: Calculate in all metabolic acidosis; use Delta-Delta to identify mixed disorders
- Correction rates: Hyponatremia and hypernatremia both require slow correction (0.25-0.5 mEq/L per hour) to avoid osmotic demyelination
- Pseudohyperkalemia: Repeat potassium in plasma (heparin tube) if hemolysis, thrombocytosis, or leukocytosis present
- Albumin correction: Always correct calcium for serum albumin before determining aggressiveness of supplementation
- Renal function: Tailor electrolyte replacement aggressiveness to renal function; aggressive repletion in ESRD causes harm
- Underlying cause: Treating the root disorder is always more important than just correcting numbers
Hematology Survival Guide
Evaluation of Bleeding Disorders
Hemostasis Physiology
Bleeding control involves a coordinated series of processes that work together to form stable clots:
Primary hemostasis involves platelets forming the initial plug through three sequential steps:
- Adhesion - vWF molecules bridge platelets to exposed subendothelium via GP Ib receptors
- Activation - Platelets receive signals through thromboxane A2 (TXA2) and ADP release
- Aggregation - GP IIb/IIIa receptors cross-link platelets together using fibrinogen as the bridge
Secondary hemostasis creates the fibrin scaffold that stabilizes the platelet plug. The coagulation cascade is organized into three interconnected pathways:
- Extrinsic pathway - Tissue factor + Factor VII activate Factor X (fastest, 5 seconds)
- Common pathway - Factors I, II, V, and X complete clot formation
- Intrinsic pathway - Factors XII, XI, IX, and VIII activate Factor X (slower, 1-2 minutes)
Factor X serves as the critical convergence point where extrinsic and intrinsic pathways merge. The final reaction produces fibrin monomers that polymerize into cross-linked clots. Plasmin later breaks down fibrin into D-dimer fragments, enabling fibrinolysis.

Antiplatelet and Anticoagulant Agents
| Agent | Mechanism | Pathway Affected | Duration |
|---|---|---|---|
| Aspirin | Irreversible TXA2 synthesis inhibition | Primary hemostasis | 7-10 days |
| Clopidogrel | ADP receptor antagonism | Primary hemostasis | 5-7 days |
| Dipyridamole | Phosphodiesterase inhibition | Primary hemostasis | Hours |
| Warfarin | Vitamin K antagonism (Factors II, VII, IX, X, Proteins C & S) | Extrinsic + Common | 3-5 days |
| Fondaparinux | Indirect Factor Xa inhibition via ATIII | Common | 2-4 days |
| Apixaban | Direct Factor Xa inhibition | Common | 12-24 hours |
| Rivaroxaban | Direct Factor Xa inhibition | Common | 24 hours |
| Dabigatran | Direct thrombin (IIa) inhibition | Common | 24-36 hours |
| Lepirudin | Direct thrombin (IIa) inhibition | Common | Hours |
| Argatroban | Direct thrombin (IIa) inhibition | Common | Hours |
Clinical Evaluation Algorithm
The pattern of abnormal laboratory results guides diagnosis of hemostatic defects:

Mixing Studies
Mixing studies help differentiate between factor deficiencies and inhibitors:
Mixing Study Interpretation
When a patient's prolonged PT or PTT is investigated:
- Corrects after mixing with normal plasma → Factor deficiency (supply missing factor)
- Remains prolonged after mixing → Inhibitor present (antibody against factor VIII, IX, XI, or XII)
This distinction guides treatment. Factor deficiencies may benefit from replacement therapy, while inhibitors require immune suppression or bypass agents.
Anticoagulant Reversal
Reversal Strategies
| Anticoagulant | Acute Reversal Agent(s) | Dosing | Notes |
|---|---|---|---|
| Warfarin | Vitamin K IV | 2.5-5 mg (stable INR 4.5-10); 10 mg (INR >10) | Onset 12-24h; hold warfarin first |
| KCentra (Prothrombin Complex Concentrate) | 1,500-2,000 units IV | Immediate effect; preferred for active bleeding | |
| FFP | 2-4 units IV | Last resort if KCentra unavailable | |
| Apixaban/Rivaroxaban | Andexanet Alfa | Weight/dose-based bolus + infusion | Specific reversal; FDA approved |
| KCentra | 50 units/kg IV | Reasonable alternative | |
| Tranexamic acid | 1-1.5 g PO q8h | Consider as adjunct | |
| Dabigatran | Idarucizumab | 2-5 mg IV q10 minutes × 2 doses | Specific monoclonal; FDA approved |
| Emergent hemodialysis | N/A | Dabigatran is dialyzable | |
| Tranexamic acid | 1-1.5 g PO q8h | Consider as adjunct | |
| Unfractionated Heparin | Protamine Sulfate | 1 mg per 100 units heparin | Dose adjusted by time since last dose |
| Given as slow IV infusion | Monitor PTT 5 minutes after | ||
| Low-Molecular-Weight Heparin | Protamine Sulfate | 1 mg per 100 units LMWH | Partial neutralization only (~60%) |
| Give slowly IV | Repeat dose q2-4h if needed | ||
| Aspirin | Platelet Transfusion | 1 unit (or pool of 6) | Temporary effect |
| Consider for active bleeding only | Effective for 3-7 days post-aspirin | ||
| Clopidogrel | Platelet Transfusion | 1 unit (or pool of 6) | Similar to aspirin |
| DDAVP | 0.3 mcg/kg IV | For platelet dysfunction/uremia |
Clinical INR Management (Warfarin)
INR-Based Warfarin Management
INR 4.5-10 without bleeding:
- Hold warfarin doses and recheck INR in 2-4 days
- No immediate reversal needed
INR >10 without bleeding:
- Hold warfarin
- Give vitamin K 2.5-5 mg orally (slower, safer) or IV (faster but higher reversal risk if over-correcting)
- Recheck INR in 12-24 hours
- Consider KCentra if urgent surgery planned
Active bleeding at any INR:
- STAT: Vitamin K 10 mg IV slow infusion + KCentra 1,500-2,000 units IV
- Recheck INR 15-30 minutes after
- May repeat KCentra if still elevated
Perioperative Anticoagulation Holding Times
| Anticoagulant | Hold Before Surgery | Resume After Surgery |
|---|---|---|
| Warfarin | 5 days (INR <1.5) | Evening of surgery or day 1 |
| Apixaban | 2-3 days | 24 hours if low bleeding risk; 48h if high |
| Rivaroxaban | 2-3 days | 24 hours if low bleeding risk; 48h if high |
| Dabigatran | 2-5 days | 24 hours if low bleeding risk; 48h if high |
| Aspirin | 5-7 days | Resume per procedure protocol |
| Clopidogrel | 5-7 days | Resume per procedure protocol |
| Unfractionated Heparin | Stop 4-6 hours preop | Resume within 24 hours postop |
| LMWH | Last dose 24 hours preop | Resume 24-48 hours postop |
Leukocytosis
Normal WBC Differential
| Cell Type | Normal Range | Associated Conditions |
|---|---|---|
| Neutrophils | 40-60% (2.0-7.5 K/μL) | Infection, inflammation, stress response, malignancy, medications (corticosteroids), tobacco use, splenectomy, leukemias |
| Lymphocytes | 20-40% (1.0-4.5 K/μL) | Viral infections, pertussis, leukemias, hypersensitivity reactions, chronic infections (TB, brucellosis) |
| Monocytes | 2-8% (0.1-0.8 K/μL) | Autoimmune diseases, chronic infections (tuberculosis, fungi), splenectomy, monocytic leukemias |
| Eosinophils | 1-4% (0-0.4 K/μL) | Allergic conditions, parasitic infections, eosinophilic esophagitis, malignancies (Hodgkin lymphoma), drug reactions, eosinophilic syndromes |
| Basophils | 0.5-1% (0-0.1 K/μL) | Allergic reactions, myeloproliferative neoplasms, leukemias |
Left Shift and Immature Cells
A left shift describes the appearance of immature neutrophils (bands, metamyelocytes, myelocytes) in the peripheral blood. This indicates:
- Accelerated bone marrow release in response to infection or severe inflammation
- Typically accompanies moderate to severe leukocytosis
- Suggests acute bacterial infection, sepsis, or acute leukemia
When to Suspect Leukemia
If the differential reveals blast cells (immature myeloid or lymphoid precursors):
- Contact hematology/oncology immediately
- Do not delay bone marrow biopsy
- Flow cytometry should be obtained for definitive classification
- Avoid unnecessary transfusions (may precipitate leukostasis)
Anemia
Definition and Clinical Features
Anemia is defined as hemoglobin concentration below 12 g/dL in women or 14 g/dL in men. Clinical severity depends on acuity of onset and compensatory capacity.
Common presenting symptoms:
- Fatigue and weakness
- Dyspnea on exertion (or at rest if severe)
- Chest pain or angina (especially in CAD patients)
- Pallor of conjunctivae, palms, and nail beds
- Tachycardia and tachypnea
- Orthostatic hypotension
- Jaundice (suggests hemolysis)
- Splenomegaly (hemolysis, leukemia, cirrhosis)
Initial Diagnostic Approach
The workup of anemia follows a systematic algorithm:
- Complete blood count with differential - platelet count, WBC, hemoglobin, hematocrit
- RBC indices and reticulocyte count - Mean Corpuscular Volume (MCV), Mean Corpuscular Hemoglobin (MCH), Mean Corpuscular Hemoglobin Concentration (MCHC), Reticulocyte Index
- Peripheral blood smear - RBC morphology, white cell abnormalities, platelets
- Iron studies - serum iron, total iron-binding capacity (TIBC), ferritin, transferrin saturation
- Hemolysis markers if indicated - LDH, haptoglobin, indirect bilirubin, direct antiglobulin test (Coombs)
- Consider additional testing - B12, folate, TSH, renal function, liver function
Understanding RBC Parameters
| Parameter | Meaning | Clinical Correlation |
|---|---|---|
| Hemoglobin (Hgb) | Total hemoglobin concentration in whole blood (g/dL) | Primary measure of oxygen-carrying capacity |
| Hematocrit (Hct) | Fraction of blood volume occupied by intact RBCs (%) | Roughly equals Hgb × 3 |
| MCV | Average RBC volume (fL) | Classifies anemia (micro/normo/macrocytic) |
| MCH | Average hemoglobin content per RBC (pg) | Low = hypochromic |
| MCHC | Average hemoglobin concentration in RBCs (%) | High = spherocytes; low = hypochromia |
| RDW | Distribution width reflecting RBC size variation (%) | High = anisocytosis; broad size variation |
Quick RBC Math
- RBC count × 3 ≈ Hemoglobin
- Hemoglobin × 3 ≈ Hematocrit
Use these to quickly verify lab values for internal consistency.
Urgent Clinical Scenarios
Urgent Hematology Situations
- Acute hemorrhage - massive transfusion protocol activation, ICU monitoring
- Microangiopathic hemolytic anemia (MAHA) - disseminated intravascular coagulation, hemolytic uremic syndrome, thrombotic thrombocytopenic purpura
- Sickle cell crisis - vaso-occlusive crisis, acute chest syndrome, splenic sequestration
- Severe leukemias - blast crisis, severe cytopenia, risk of leukostasis
- Aplastic anemia - pancytopenia with infection risk, hemorrhage risk
Microcytic Anemia (MCV <80)
Iron Deficiency Anemia
Iron deficiency represents the most common cause of microcytic anemia worldwide. Progressive depletion of iron stores impairs hemoglobin synthesis.
Laboratory features:
- Low serum iron, elevated TIBC, low ferritin, low transferrin saturation
- Peripheral smear shows hypochromic microcytic RBCs with possible target cells
- RDW typically elevated (high variation in RBC size)
Clinical signs of chronic iron deficiency:
- Angular cheilosis (cracks at mouth corners)
- Pica (craving non-food items)
- Koilonychia (spoon-shaped nails)
- Atrophic glossitis (tongue atrophy)
Plummer-Vinson syndrome represents severe chronic iron deficiency with the triad of iron deficiency anemia, esophageal webs, and atrophic glossitis. This carries increased risk of esophageal carcinoma and must be monitored closely.
Treatment:
- Oral ferrous sulfate 325 mg every 48 hours (GI upset limits daily dosing)
- Pair with vitamin C to enhance absorption
- IV iron formulations available for severe deficiency, malabsorption, or intolerance to oral therapy
- Expect reticulocyte response in 3-7 days, Hgb improvement in 3-6 weeks
- Identify and treat underlying cause (GI bleeding, poor dietary intake, malabsorption)
Thalassemia
Thalassemias result from genetic deletions or mutations affecting globin chain production, leading to imbalanced hemoglobin synthesis. Two main types exist:
Alpha-thalassemia - deletions on chromosome 16 affecting alpha-globin genes: - Prevalence in Southeast Asian, Mediterranean, and African populations - Severity ranges from silent carrier to Hb H disease to hydrops fetalis - Diagnosis requires careful clinical suspicion; gene testing confirms mutations
Beta-thalassemia - mutations on chromosome 11 affecting beta-globin genes: - Prevalence in Mediterranean, African, and Asian populations - Thalassemia major (homozygous) presents in infancy with severe hemolytic anemia - Thalassemia minor (heterozygous) presents as mild microcytic anemia - Hemoglobin electrophoresis shows elevated HbA2 and/or HbF
Laboratory differentiation from iron deficiency: - Normal or elevated serum iron and ferritin (from chronic transfusions) - Normal or low TIBC - Normal or increased RBC count (contrasts with iron deficiency)
Anemia of Chronic Disease
This represents the second most common cause of anemia after iron deficiency. Chronic inflammation impairs iron utilization and erythropoietin responsiveness.
Associated conditions:
- Autoimmune diseases (rheumatoid arthritis, systemic lupus erythematosus)
- Chronic infections (tuberculosis, osteomyelitis, endocarditis)
- Malignancies (both from tumor burden and chemotherapy)
- End-stage renal disease
Laboratory pattern:
- Low serum iron, low TIBC, normal or elevated ferritin
- Contrasts with iron deficiency (which shows high TIBC)
- Generally mild to moderate severity
- May be normocytic or microcytic
Management:
- Treat underlying disease
- Erythropoiesis-stimulating agents for renal disease or chemotherapy-induced anemia
- Iron supplementation often unhelpful in pure anemia of chronic disease
Sideroblastic Anemia
Rare disorder characterized by abnormal iron accumulation in mitochondria, creating pathognomonic findings on bone marrow examination.
Microscopic features:
- Pappenheimer bodies - iron-laden mitochondria visible on bone marrow biopsy
- Ring sideroblasts - myeloblasts with iron-laden rings surrounding the nucleus
- Typically presents with microcytic or normocytic anemia
Causes include:
- Myelodysplastic syndrome (most common acquired form)
- Copper deficiency
- Medications (isoniazid, chloramphenicol, linezolid)
- Alcohol abuse
- Idiopathic or X-linked inheritance
Normocytic Anemia (MCV 80-100)
Aplastic Anemia
Aplastic anemia represents bone marrow failure with severely reduced hematopoietic progenitor cells. The hallmark is pancytopenia with absent reticulocyte response.
Laboratory findings:
- Low hemoglobin, low platelet count, low WBC
- Reticulocyte count inappropriately low (not elevated despite anemia)
- Peripheral smear shows normal RBC morphology
- Bone marrow biopsy shows hypocellular marrow with fat spaces
Common etiologies:
- Idiopathic (most common; autoimmune mechanism suspected)
- Radiation or chemotherapy exposure
- Viral infections (EBV, parvovirus B19, HIV)
- Medications (chloramphenicol, NSAIDs, anticonvulsants, sulfonamides)
- Autoimmune diseases
Management:
- Supportive care with transfusions
- Immunosuppressive therapy (ATG, cyclosporine)
- Hematopoietic stem cell transplantation if available and younger patient
- Avoid unnecessary transfusions that may allo-sensitize before transplant
Hemolytic Anemia
Hemolytic anemias result from shortened RBC lifespan (normal ~120 days). Bone marrow appropriately increases erythropoiesis, creating elevated reticulocyte count.
Laboratory hallmarks of hemolysis:
- Elevated reticulocyte count (>2%)
- Elevated LDH (from RBC destruction)
- Low haptoglobin (consumed binding free hemoglobin)
- Elevated indirect bilirubin (from heme degradation)
- Direct antiglobulin test (Coombs) positive or negative depending on mechanism
Immune-mediated hemolysis (Coombs positive):
- Warm autoimmune hemolytic anemia - IgG antibodies bind RBCs optimally at body temperature
- Most common autoimmune hemolytic anemia
- Associated with systemic lupus erythematosus, chronic lymphocytic leukemia, lymphomas
-
Treatment: corticosteroids (prednisone 1 mg/kg/day) or IVIG
-
Cold agglutinin disease - IgM antibodies bind RBCs optimally at cold temperatures
- Symptoms worse in cold weather
- Associated with infections (mycoplasma, EBV) or lymphomas
- Treatment: cold avoidance, rituximab, complement inhibitors
Intrinsic RBC defects (Coombs negative hemolysis):
- G6PD deficiency - most common enzyme defect worldwide
- X-linked inheritance
- Hemolytic episodes triggered by oxidative stress (fava beans, sulfa drugs, infections, aspirin)
- Peripheral smear shows Heinz bodies (precipitated hemoglobin) and bite cells (phagocytes removing Heinz bodies)
-
Diagnosis: G6PD enzyme assay; avoid hemolytic triggers
-
Sickle cell disease - polymerization of hemoglobin S
- Vaso-occlusive crises from RBC sickling in small vessels
- Acute chest syndrome (pleuritic chest pain, infiltrate)
- Splenic sequestration (sudden Hgb drop, splenomegaly, shock)
- Peripheral smear shows Howell-Jolly bodies (nuclear remnants from hyposplenism)
-
Treatment: hydroxyurea, transfusions for crises, penicillin prophylaxis
-
Hereditary spherocytosis - RBC membrane protein defects
- Spherical RBC shape with osmotic fragility (lyse in hypotonic solutions)
- Family history common
-
Treatment: folic acid supplementation, splenectomy if severe
-
Paroxysmal nocturnal hemoglobinuria (PNH) - acquired complement-mediated hemolysis
- Absent CD55 and CD59 (complement regulatory proteins) on blood cells
- Diagnosis: flow cytometry testing for CD55/CD59
- Thrombosis risk; use anticoagulation
- Treatment: complement inhibitors (eculizumab, pegcetacoplan)
Extrinsic hemolysis (Coombs negative):
- Microangiopathic hemolytic anemia (MAHA) - RBC fragmentation in small vessels
- Schistocytes (fragmented RBCs) on peripheral smear
- Associated with DIC, hemolytic uremic syndrome, thrombotic thrombocytopenic purpura
-
See separate sections on these conditions
-
Hypersplenism - pooling and destruction in enlarged spleen
- Splenomegaly from cirrhosis, leukemia, lymphoma, or infection
- Hemolysis less prominent than thrombocytopenia
-
Treatment: splenectomy if severe
-
Infection-mediated hemolysis - direct parasitic damage or immune activation
- Malaria, clostridial infection, sepsis
- Treatment: antibiotics and supportive care
Macrocytic Anemia (MCV >100)
Megaloblastic Anemias
Megaloblastic anemias result from impaired DNA synthesis affecting all rapidly dividing cells. RBC precursors become dysplastic, producing larger RBCs with asynchronous maturation.
Laboratory features:
- Hypersegmented neutrophils - >5 nuclear lobes (normal is 3-5)
- Pancytopenia possible
- Elevated LDH and elevated indirect bilirubin (ineffective erythropoiesis)
- Bone marrow shows megaloblastic changes
Vitamin B12 deficiency:
- Reduced B12 impairs methylation reactions essential for DNA synthesis
- Laboratory findings: elevated methylmalonic acid, elevated homocysteine
- Clinical manifestations include subacute combined degeneration:
- Paresthesias (peripheral neuropathy)
- Weakness and ataxia (posterior column dysfunction)
- Cognitive changes, dementia if prolonged
-
Optic neuropathy
-
Common causes:
- Pernicious anemia (autoimmune destruction of gastric parietal cells producing intrinsic factor)
- Gastrectomy or gastric bypass surgery
- Chronic metformin or proton pump inhibitor use
- Vegan diet
-
Terminal ileum disease (Crohn's disease, celiac sprue)
-
Treatment: B12 1 mg IM daily for 7 days, then weekly for 4-8 weeks, then monthly lifelong
- Oral B12 supplements (cyanocobalamin) less reliable due to absorption issues
- Neurologic symptoms may not fully reverse if long-standing
Folate deficiency:
- Folate essential for single-carbon transfer reactions and DNA synthesis
- Laboratory findings: low serum folate, elevated homocysteine, normal methylmalonic acid (unlike B12 deficiency)
- No neurologic manifestations (distinguishes from B12 deficiency)
- Common causes:
- Malnutrition
- Alcoholism
- Methotrexate or trimethoprim use
- Pregnancy
-
Hemolytic anemias (increased consumption)
-
Treatment: Folate 1 mg orally daily for 1-4 months
B12 vs. Folate Deficiency
Never give folate supplementation to a patient with unrecognized B12 deficiency. Folate can "mask" the hematologic manifestations of B12 deficiency while neurologic damage continues to progress. Always check B12 level first if suspecting either deficiency.
Non-Megaloblastic Macrocytic Anemias
Liver disease: - Cirrhosis and hepatitis impair thrombopoietin production and cause portal hypertension - Hypersplenism contributes to anemia - RBC membrane abnormalities create macrocytic indices - Treatment: address underlying liver disease
Alcoholism: - Direct toxic effect on bone marrow - Folate depletion from poor nutrition - May also cause sideroblastic changes - Treatment: abstinence, nutritional support, folate supplementation
Reticulocytosis: - Elevated reticulocyte count creates higher average RBC volume (reticulocytes larger than mature RBCs) - Occurs in response to hemolysis or acute blood loss - MCV normalizes as reticulocytes mature; this is not true pathologic macrocytosis
Hypothyroidism: - Decreased metabolic rate slows erythropoiesis - Creates mild macrocytosis - Treatment: thyroid hormone replacement
Myelodysplastic syndromes: - Dysplastic changes in hematopoietic precursors - Macrocytic anemia common - Risk of progression to acute leukemia - Treatment: supportive care, azacitidine for higher-risk MDS
Thrombocytopenia
Clinical Thresholds
When evaluating thrombocytopenia, the absolute platelet count guides assessment of bleeding and thrombosis risk:
| Platelet Count | Spontaneous Bleeding Risk | Clinical Significance |
|---|---|---|
| >100 K/μL | Minimal | Normal hemostasis |
| 50-100 K/μL | Low; only with major trauma | Acceptable for most procedures |
| 20-50 K/μL | Minor bleeding with trauma | Increased concern with invasive procedures |
| <20 K/μL | Spontaneous bleeding possible | Major hemorrhage risk |
| <10 K/μL | Significant spontaneous bleeding | Life-threatening; transfuse immediately |
Thrombotic Thrombocytopenia Alert
Certain conditions cause thrombocytopenia with paradoxical thrombosis risk:
- HIT (Heparin-Induced Thrombocytopenia) - prothrombotic state despite low platelets
- Antiphospholipid syndrome - thrombosis despite thrombocytopenia
- DIC - simultaneous coagulation consumption
- TTP - microthrombi formation
- PNH - high thromboembolism risk
These require specific evaluation and anticoagulation, not just transfusion support.
Diagnostic Approach
The workup of new-onset thrombocytopenia should distinguish decreased production from increased destruction or sequestration:
Initial investigations:
- CBC with differential - confirm thrombocytopenia, assess hemoglobin and WBC
- Peripheral blood smear - rule out pseudothrombocytopenia (platelet clumping), assess RBC/WBC morphology
- HIV and HCV serology - common infectious causes
- Direct antiglobulin test (Coombs) - assess for concurrent hemolytic anemia
Additional testing based on clinical context:
- Viral titers (EBV, CMV, HSV) - if infectious cause suspected
- Flow cytometry - assess for immune-mediated destruction, PNH
- ANA and antiphospholipid antibodies - autoimmune/vasculitis assessment
- LDH, haptoglobin, indirect bilirubin, schistocytes - hemolysis markers
- PT, PTT, fibrinogen, D-dimer - coagulation assessment for DIC
- Bone marrow biopsy - if production defect suspected or diagnosis unclear
Immune Thrombocytopenia (ITP)
ITP represents autoimmune destruction of platelets by circulating IgG antibodies targeting platelet surface glycoproteins (usually GP IIb/IIIa or GP Ib/IX).
Diagnostic criteria:
- Diagnosis of exclusion after ruling out secondary causes
- Isolated thrombocytopenia (no other cytopenias)
- Normal bone marrow with adequate megakaryocytes
- Absence of clinical splenomegaly
- No family history of thrombocytopenia
Classification:
- Newly diagnosed - <3 months duration
- Persistent - 3-12 months duration
- Chronic - >12 months duration
Treatment approach:
- Mild asymptomatic thrombocytopenia (>20 K) - observation
- Symptomatic or platelets <20 K:
- First-line: Corticosteroids (prednisone 1 mg/kg/day) or IVIG (2 g/kg over 3-5 days)
- Response rates: 70-80% with steroids, 80-90% with IVIG
-
IVIG preferred if rapid platelet elevation needed (more rapid onset)
-
Refractory or relapsed disease:
- Rituximab (monoclonal anti-CD20 antibody)
- Splenectomy (70% response rate; effect lasts 5+ years in 80%)
- Thrombopoietin receptor agonists (romiplostim, eltrombopag)
Microangiopathic Hemolytic Anemia (MAHA)
Hemolytic Uremic Syndrome (HUS)
HUS results from Shiga toxin produced by certain bacteria (most commonly Escherichia coli O157:H7, also Shigella). The toxin damages microvascular endothelium, triggering the characteristic triad:
Classic triad:
- Thrombocytopenia - platelet consumption in microthrombi
- Microangiopathic hemolytic anemia - mechanical fragmentation of RBCs passing through narrowed vessels
- Acute renal failure - glomerular capillary damage
Laboratory findings:
- Schistocytes on peripheral smear (fragmented RBCs)
- Elevated creatinine and oliguria (renal dysfunction)
- Normal PT/PTT/fibrinogen (distinguishes from DIC)
- Elevated LDH, low haptoglobin, elevated indirect bilirubin (hemolysis markers)
Clinical presentation:
- Often follows diarrheal illness (often bloody diarrhea from Shiga toxin enteritis)
- Younger children most severely affected
- Fever may precede hemolysis and thrombocytopenia
- Neurologic symptoms less prominent than in TTP
Management:
- Supportive care is cornerstone of therapy
- Fluid management and renal replacement therapy as needed
- DO NOT routinely transfuse platelets (may worsen thrombosis)
- Prognosis excellent in children; worse in adults
- Antibiotics for underlying infection (though post-diarrheal HUS prognosis often good regardless)
Thrombotic Thrombocytopenic Purpura (TTP)
TTP results from severely deficient ADAMTS13 activity (either congenital or from acquired inhibitory antibodies). Uncleaved vWF multimers cause widespread platelet aggregation and microvascular thrombosis.
Classic pentad (full pentad rare; thrombocytopenia + MAHA sufficient for diagnosis):
- Fever - occurs in 25-50%
- Microangiopathic hemolytic anemia - mechanical fragmentation
- Thrombocytopenia - severe, often <20 K
- Renal dysfunction - occurs in ~50% (usually mild compared to HUS)
- Neurologic symptoms - most distinctive feature (50-60%)
- Fluctuating mental status, confusion, delirium
- Seizures
- Focal neurologic deficits (stroke-like)
- Often neurologic symptoms precede other manifestations
Laboratory findings:
- Schistocytes on smear
- Severe thrombocytopenia
- Severe hemolysis (very elevated LDH, very low haptoglobin)
- Normal PT/PTT/fibrinogen (CRITICAL distinction from DIC)
- ADAMTS13 activity <10% confirms diagnosis
Management - URGENT PLASMA EXCHANGE:
TTP Treatment Protocol
IMMEDIATE actions:
- Start plasma exchange within hours of diagnosis
- Goal: remove autoantibodies against ADAMTS13 and replace enzyme activity
- Continue daily plasma exchange until platelet recovery (may require 5-15 days)
- DO NOT GIVE PLATELETS or FFP unless life-threatening hemorrhage (may worsen thrombosis)
- Add corticosteroids (methylprednisolone 1 g IV daily) as adjunctive therapy
Expected response:
- Platelet recovery within 3-5 days with appropriate therapy
- Failure to respond to plasma exchange suggests alternative diagnosis
- Rituximab or other immunotherapy for ADAMTS13 inhibitor-mediated cases
Disseminated Intravascular Coagulation (DIC)
DIC represents pathologic activation of the coagulation cascade in response to severe systemic illness. Widespread fibrin formation consumes coagulation factors and platelets while simultaneously activating fibrinolysis, creating a bleeding diathesis.
Pathophysiology:
Tissue damage or endotoxin triggers Tissue Factor exposure → activation of the extrinsic pathway → widespread thrombin generation → fibrin clot formation throughout the microvasculature → consumption of factors, fibrinogen, and platelets → compensatory fibrinolysis → D-dimer elevation
Triggering conditions:
- Massive trauma (especially head trauma)
- Sepsis (bacterial endotoxins most common)
- Malignancies (especially acute leukemias, prostate cancer)
- Obstetric complications (placental abruption, amniotic fluid embolism, retained dead fetus syndrome)
- Severe hemolysis
- Acute liver failure
- Snake bite
- Heatstroke
Laboratory diagnostic criteria (at least 2 required):
- Thrombocytopenia (usually moderate, platelet count 50-100 K)
- Low fibrinogen (<100 mg/dL) - consumed by excessive clotting
- Elevated PT/PTT - consumed factors
- Elevated D-dimer - from active fibrinolysis
- Schistocytes on peripheral smear - mechanical hemolysis
Clinical presentation:
- Acute DIC - fulminant bleeding (cutaneous, GI, pulmonary)
- Chronic DIC - milder consumptive coagulopathy (seen with malignancies)
- Microvascular thrombosis causing organ dysfunction
- Renal failure, respiratory distress, altered mental status
Management:
- Treat underlying cause - source control, antibiotics for sepsis, delivery for obstetric DIC
- Supportive transfusion:
- Platelets to maintain >50 K
- FFP to replace consumed factors
- Cryoprecipitate (goal fibrinogen >100 mg/dL) - fibrinogen depleted most rapidly
-
Packed RBCs for anemia from both bleeding and hemolysis
-
Anticoagulation considerations - controversial; heparin sometimes used to prevent further consumption, but bleeding risk prohibits routine use
- Monitor closely - recheck CBC, coagulation studies, fibrinogen q6-12h during acute phase
DIC vs. TTP Distinction
Both present with thrombocytopenia and schistocytes, but:
- DIC: Prolonged PT/PTT, low fibrinogen, high D-dimer → coagulation activation + fibrinolysis
- TTP: Normal PT/PTT/fibrinogen → normal coagulation studies, ADAMTS13 deficiency
TTP demands plasma exchange; DIC demands treating underlying cause.
Heparin-Induced Thrombocytopenia (HIT)
HIT represents a paradoxical prothrombotic state triggered by antibodies against the heparin-platelet factor 4 (PF4) complex. Despite thrombocytopenia, patients face high risk of thrombosis.
Pathophysiology
Heparin exposure causes some patients to develop IgG antibodies against complexes of heparin and platelet factor 4 (a protein released from platelet granules). These immune complexes bind to platelet Fc receptors, triggering platelet activation, microthrombi formation, and paradoxically severe thromboembolism despite low platelet counts.
4Ts Scoring System
The 4Ts score stratifies HIT probability and guides initial management decisions:
| Factor | 2 Points | 1 Point | 0 Points |
|---|---|---|---|
| Timing of platelet drop | Day 5-10 post-heparin | Day >10 or <4 (if re-exposed) | Day <4 (no prior heparin) |
| Magnitude of platelet decline | >50% drop, not below 100K | 30-50% drop or nadir 100-150K | <30% drop or nadir >150K |
| Thrombosis | New thrombosis or thromboembolism | Progressive or recurrent thrombosis during heparin | None |
| alTernative causes | None apparent | Possible | Definite alternative diagnosis |
Risk stratification:
- Score 4-5: Intermediate probability - further testing warranted
- Score 6-8: High probability - immediate action required
Diagnosis and Testing
- Clinical diagnosis based on 4Ts score
- HIT antibody assay (ELISA) - sensitive but not specific
- Platelet aggregation study - more specific; confirms functional platelet activation
- Serotonin release assay - gold standard; detects antibodies causing platelet activation
Management
HIT Management Principles
IMMEDIATELY upon HIT suspicion:
- STOP all heparin products (including heparin flushes, heparin-bonded catheters)
- Start direct thrombin inhibitor: argatroban (preferred), lepirudin, or fondaparinux
- DO NOT use warfarin monotherapy (risk of warfarin-induced skin necrosis from Protein C depletion)
Transition to warfarin:
- Bridge with direct thrombin inhibitor until INR 2-3 × 24 hours
- Then discontinue direct thrombin inhibitor and continue warfarin monotherapy
Duration of anticoagulation:
- If thrombosis occurred: ≥3-6 months
- If no thrombosis: 1-3 months
Lifelong consideration:
- Permanent avoidance of all heparin products (unfractionated heparin, LMWH)
- Document in medical record
- Patient should wear medical alert bracelet
Transfusion Management
Transfusion Indications
| Blood Product | Indication | Target Level | Notes |
|---|---|---|---|
| Packed Red Blood Cells | Symptomatic anemia or acute hemorrhage | Hgb ~7-10 g/dL depending on clinical context | 1 unit raises Hgb ~1 g/dL, Hct ~3% |
| Platelets | <10 K always; <20 K if bleeding; <50 K before surgery | Maintain >20 K if active bleeding | 1 unit raises platelets ~30 K (depends on patient factors) |
| Fresh Frozen Plasma | Coagulopathy with bleeding, INR reversal, TTP | Depends on indication | Contains all clotting factors |
| Cryoprecipitate | Low fibrinogen, hyperfibrinolysis | Goal fibrinogen >100 mg/dL | Rich in fibrinogen and Factor XIII |
Massive Transfusion Protocol
When patients require >3 units packed RBCs in 24 hours, activate massive transfusion protocol to avoid dilutional coagulopathy:
Empiric ratio approach:
- 3:1:1 ratio - 3 units packed RBCs : 1 unit FFP : 1 six-pack platelets
- Continue this ratio until bleeding controlled
- Recheck CBC, PT/PTT, fibrinogen after every 10 units pRBC
Monitoring parameters:
- Serum ionized calcium - transfusions contain citrate anticoagulant that can chelate calcium
- Core temperature - massive transfusion of cold blood causes hypothermia and coagulopathy
- Lactate - tissue hypoxia from inadequate resuscitation
- Hemoglobin/hematocrit
- Coagulation studies (PT, PTT, fibrinogen, D-dimer)
Transfusion Reactions
Febrile Transfusion Reaction
Fever developing during or shortly after transfusion (usually due to WBC antibodies or cytokine release):
- Stop transfusion immediately
- Send blood back to blood bank for testing
- Assess for sepsis
- Give acetaminophen and diphenhydramine
- May resume transfusion after excluding serious complications (sepsis, hemolysis)
Anaphylactic Reaction
Severe immediate reaction (usually in IgA-deficient patients transfused with IgA-containing products):
Immediate management:
- Stop transfusion immediately
- Send blood and patient samples to blood bank
- Give acetaminophen + diphenhydramine + methylprednisolone IV
- Epinephrine 0.3-0.5 mg IM every 10-15 minutes if true anaphylaxis with hypotension
- Secure airway if laryngeal edema develops; intubate early to avoid difficult airway
- Avoid repeat transfusion with standard products (use IgA-depleted products in future)
Transfusion-Related Acute Lung Injury (TRALI)
Immune-mediated pulmonary edema developing during or within 6 hours of transfusion. Represents one of the most serious transfusion complications.
Clinical presentation:
- Acute respiratory distress (within minutes to hours)
- Hypoxemia
- Bilateral infiltrates on chest X-ray (pulmonary edema)
- Hypertension or hypotension
- Fever, chills
Management:
- STOP transfusion immediately
- Send blood to blood bank for testing
- Obtain CXR - shows bilateral infiltrates consistent with ARDS
- Rule out volume overload or other causes of acute respiratory distress
- Methylprednisolone IV as adjunctive therapy
- Oxygen supplementation; support oxygenation aggressively
- Intubate early with sustained PEEP rather than delaying
- Most patients recover within 48-96 hours with supportive care
- Avoid repeat transfusion from implicated donors
Key Clinical Pearls
Hematology Practice Tips
-
Reticulocyte count is your friend - appropriately elevated in hemolysis, appropriately low in aplastic anemia; tells you if marrow is responding
-
Always check a smear - computerized WBC counts miss blasts, abnormal morphology, clues to diagnosis
-
Mixing study timing matters - perform immediately; delays cause in vitro factor activation/degradation
-
PT/PTT patterns guide diagnosis:
- Isolated PT prolongation = Factor VII deficiency (rarest single factor deficiency)
- Isolated PTT prolongation = Intrinsic pathway defect (very common)
-
Both prolonged = Common pathway, vitamin K deficiency, or severe deficiency of multiple factors
-
Warfarin reversal is time-dependent - vitamin K takes 12-24 hours; use KCentra for urgent bleeding
-
DOACs are more reversible than you think - andexanet alfa and idarucizumab are specific antidotes with good efficacy
-
HIT is prothrombotic, not just thrombocytopenic - stop heparin immediately, start direct thrombin inhibitor, avoid platelets/FFP
-
TTP demands plasma exchange NOW - mortality >90% untreated; >90% survive with plasma exchange
-
Never assume bleeding is from low platelets - coagulopathy and platelet dysfunction matter too
-
Document anticoagulation holding times - surgery requires specific lead times; don't just restart on postop day 1
Quick Reference Tables
Hemostasis Laboratory Values
| Test | Normal Range | Interpretation |
|---|---|---|
| PT (INR) | 0.8-1.1 (INR) | Prolongation suggests Factors II, V, VII, X or fibrinogen deficiency |
| aPTT | 25-35 seconds | Prolongation suggests intrinsic pathway or common pathway defect |
| Fibrinogen | 200-400 mg/dL | Low in DIC, liver disease, massive transfusion |
| Platelet Count | 150-400 K/μL | <50 K increases bleeding risk; <20 K high spontaneous bleeding risk |
| D-dimer | <500 ng/mL | Elevated in DIC, VTE, sepsis, recent surgery |
| Haptoglobin | 30-200 mg/dL | Low in hemolysis (consumed binding free Hgb) |
| LDH | 140-280 IU/L | Elevated in hemolysis, liver disease, myocardial infarction |
| Indirect Bilirubin | 0.1-0.3 mg/dL | Elevated in hemolysis (heme breakdown) |
| Reticulocyte Count | 0.5-2.5% | Elevated response to anemia or hemolysis; inappropriately low in aplastic anemia |
MCV-Based Anemia Classification Quick Reference
| MCV Range | Likely Diagnoses | Next Step |
|---|---|---|
| <80 (Microcytic) | Iron deficiency, thalassemia, anemia of chronic disease, sideroblastic | Iron studies; Hgb electrophoresis if indicated |
| 80-100 (Normocytic) | Aplastic anemia, hemolytic anemia, acute hemorrhage, chronic kidney disease | Reticulocyte count; peripheral smear; hemolysis labs |
| >100 (Macrocytic) | B12 deficiency, folate deficiency, liver disease, hypothyroidism, MDS | B12 and folate levels; LFTs; TSH |
Cardiology
Chest Pain Assessment and Acute Coronary Syndrome
Understanding Chest Pain Etiology
Chest pain can originate from multiple anatomical structures. A systematic approach by anatomical layer helps narrow the differential diagnosis:
| Layer | Common Conditions |
|---|---|
| Skin & Subcutaneous | Laceration, herpes zoster, cellulitis |
| Musculoskeletal | Costochondritis, muscle strain, rib fractures |
| Pleural | Pleurisy, pneumothorax, pneumonia |
| Pericardium | Pericarditis, pericardial effusion, tamponade |
| Cardiac | Acute coronary syndrome, myocarditis, acute heart failure |
| Esophageal | Gastroesophageal reflux disease, esophageal spasm, perforation |
| Aortic | Aortic dissection, thoracic aortic aneurysm |
| Abdominal | Biliary colic, pancreatitis, peptic ulcer disease |
| Psychiatric | Anxiety disorder, panic attacks |
Aortic Dissection Red Flags
Don't let dissection hide among the other causes of chest pain. Two quick bedside clues:
- Blood pressure differential ≥20 mmHg between the arms
- Pulse deficit (asymmetric or absent peripheral pulses)
Pair these with tearing pain radiating to the back and a widened mediastinum on chest X-ray.
Angina Classification Systems
Diamond Classification (Typicality of Angina)
The Diamond classification helps stratify the probability that chest pain represents true anginal discomfort:
- 3 of 3 typical features: Substernal location + Provoked by exertion + Relieved by nitroglycerin or rest = Typical angina
- 2 of 3 typical features = Atypical angina
- 1 of 3 typical features = Non-anginal chest pain
Clinical Pearl
Use this classification to guide your pretest probability assessment before ordering additional diagnostic testing.
Canadian Cardiovascular Society Grading
This scale quantifies functional limitations from angina:
| Grade | Characteristics |
|---|---|
| I | Chest pain only with strenuous or prolonged exertion |
| II | Mild limitation; pain with light exertion (climbing stairs, walking >2 blocks) |
| III | Marked limitation; pain with ordinary activities (walking 1-2 blocks on flat surface) |
| IV | Unable to perform any activity without symptoms; pain at rest |
Initial Assessment and Workup
Time-Critical Actions
All chest pain patients require an EKG within 10 minutes of arrival.
Immediate Diagnostic Tests
- Electrocardiogram — obtain within 10 minutes
- Complete blood count — assess for anemia or infection
- Comprehensive metabolic panel — electrolytes, renal function, glucose
- Oxygen saturation — by pulse oximetry
- Chest radiograph — assess for alternative diagnoses
- Cardiac telemetry — continuous monitoring for arrhythmias
- Initial troponin — high-sensitivity troponin preferred
Serial Testing Protocol
- Repeat EKG at 2-3 minutes if initial is normal or nondiagnostic and clinical suspicion remains high
- Serial troponin measurements at 4-6 hour intervals for at least 2 measurements
- Troponin may be normal in the first 3 hours of symptom onset
EKG Localization of Myocardial Infarction
Understanding which coronary artery corresponds to EKG changes guides your assessment:
| EKG Leads | Myocardial Region | Likely Culprit Artery |
|---|---|---|
| V1–V2 | Septal wall | Left anterior descending |
| V3–V4 | Anterior wall | Left anterior descending |
| I, aVL | Lateral wall | Left circumflex or LCx diagonal |
| V5–V6 | Lateral wall | Left circumflex |
| II, III, aVF | Inferior wall | Right coronary artery |
| V4R | Right ventricle | Right coronary artery |
| V1–V3 (ST depression) | Posterior wall (reciprocal) | Right coronary or left circumflex |
RV Infarction Clue
If inferior STEMI is present, always check lead V4R for ST elevation suggesting right ventricular involvement.
Risk Stratification Scores
TIMI Risk Score for Unstable Angina/NSTEMI
Calculate points (0-7 total) and correlate with mortality risk:
| Criterion | Points |
|---|---|
| Age ≥65 years | 1 |
| ≥3 cardiac risk factors | 1 |
| Known CAD (stenosis ≥50%) | 1 |
| Aspirin use in past 7 days | 1 |
| ST-segment deviation ≥0.5 mm | 1 |
| Elevated cardiac biomarkers | 1 |
| Severe angina (≥2 episodes in 24h) | 1 |
Risk stratification: 0-1 points = low risk, 2-4 points = intermediate risk, 5-7 points = high risk
GRACE Risk Score
The GRACE score incorporates multiple variables to predict in-hospital and 6-month mortality. Consult scoring tools/nomograms for accurate calculation. Generally:
- Score <140 = Low risk
- Score 140–200 = Intermediate risk
- Score >200 = High risk
Understanding Troponin Elevation
Elevated cardiac troponin indicates myocardial injury but does not specify etiology:
| Type | Mechanism | Examples |
|---|---|---|
| Type 1 | Atherosclerotic plaque rupture with thrombosis | STEMI, NSTEMI |
| Type 2 | Myocardial supply-demand mismatch | Sepsis, anemia, hypertensive crisis, tachyarrhythmia, hypoxia |
| Non-MI elevation | Other myocardial processes | Heart failure, myocarditis, renal failure, pulmonary embolism, sepsis |
Critical Insight
Elevated troponin requires correlation with clinical context, EKG findings, and imaging to determine true MI versus other causes of myocardial injury.
Approaching a Suspected Type 2 MI
Type 2 MI is very common in hospitalized patients — supply–demand mismatch from sepsis, anemia, hypoxia, or tachyarrhythmia. Don't anchor on it too early:
- Confirm it is not Type 1 — look for ischemic symptoms, dynamic EKG changes, and a rising/falling troponin.
- Identify the trigger and address the cause — infection, anemia, hypoxia, arrhythmia, or hemodynamic instability.
- Risk stratify for underlying CAD — review history, symptoms, and EKG; consult cardiology if the diagnosis is uncertain.
- Document the rationale supporting a Type 2 (rather than Type 1) myocardial infarction.
Stress Testing Modalities
| Test Type | Indications | Limitations |
|---|---|---|
| Exercise stress test | Intermediate pretest probability, interpretable EKG, able to exercise | Cannot perform if unable to exercise; unreliable with baseline EKG abnormalities |
| Pharmacologic stress (adenosine/regadenoson) | Unable to exercise, need imaging component | Contraindicated in severe asthma/COPD (adenosine) |
| Dobutamine stress echo | Unable to exercise, need structural assessment | Induces demand ischemia; contraindicated in uncontrolled HTN or tachyarrhythmia |
| Coronary CTA | Low-intermediate pretest probability, assess for alternative diagnosis | Radiation exposure, contrast allergy risk, poor image quality with high heart rate |
Acute Coronary Syndrome Treatment
STEMI Protocol
Time is Myocardium
Door-to-balloon time goal: <90 minutes for primary percutaneous coronary intervention.
Immediate management:
- Aspirin — 325 mg (loading), then 81 mg daily indefinitely
- Anticoagulation — unfractionated heparin IV bolus/drip or enoxaparin 0.5 mg/kg IV bolus
- Beta-blocker — if HR >50 and SBP >90 mmHg
- Nitroglycerin — 0.4 mg sublingual, repeat every 5 minutes as needed for symptom relief
- Primary PCI — mechanical revascularization within 90 minutes, or
- Fibrinolysis — if PCI unavailable; initiate within 30 minutes (thrombolytic agents: alteplase, reteplase, tenecteplase)
Accepting a STEMI From the ED
If you are accepting a patient with ST elevation and ongoing chest pain, confirm that cardiology has already been consulted. You may be taking the call away from your senior — let the ED know you will discuss the case with your senior and call back as soon as possible.
NSTEMI/Unstable Angina Treatment
Medical management:
- Aspirin — 325 mg loading dose, then 81 mg daily
- P2Y12 inhibitor — clopidogrel 600 mg loading (then 75 mg daily), prasugrel, or ticagrelor
- Anticoagulation — unfractionated heparin drip or LMWH (enoxaparin 1 mg/kg SQ BID)
- Oxygen — only if SaO2 <90%
- Nitroglycerin — 0.4 mg sublingual every 5 minutes, transition to IV infusion if ongoing symptoms
- Beta-blocker — (hold if HR <55 or SBP <100)
- High-intensity statin — atorvastatin 80 mg daily or rosuvastatin 40 mg daily
- ACE inhibitor/ARB — initiate at 1-2 days post-infarction if tolerated
Invasive Strategy
Most NSTEMI patients benefit from early invasive evaluation (cardiac catheterization within 12-72 hours depending on risk stratification).
Let the GRACE Score Drive NSTEMI Disposition
Calculate the GRACE score on every NSTEMI and include it when you call cardiology (decision cutoff 140):
- GRACE <140 overnight — you can start the ACS protocol and consult cardiology in the morning.
- GRACE ≥140 — cardiology should be consulted urgently, within 2–12 hours.
Heart Failure: Classification and Management
Heart Failure Types and Definitions
Heart failure is classified along multiple dimensions:
Ejection Fraction-Based Classification
| Classification | EF Range | Pathophysiology |
|---|---|---|
| HFrEF (reduced) | <40% | Systolic dysfunction; dilated ventricle with poor contractility |
| HFmrEF (mildly reduced) | 40–49% | Intermediate systolic function |
| HFpEF (preserved) | ≥50% | Diastolic dysfunction; normal EF but impaired filling |
Structural Classification
- Systolic HF: Decreased contractility; EF typically <40%
- Diastolic HF: Preserved contractility; impaired relaxation or increased stiffness
Output Classification
- Forward failure: Inadequate perfusion to organs (low cardiac output)
- Backward failure: Venous congestion upstream of failing ventricle
- High-output failure: Excessive metabolic demand (sepsis, thyrotoxicosis, anemia, pregnancy)
NYHA Functional Classification and Treatment Strategy
| Class | Description | Symptoms | Baseline Treatment |
|---|---|---|---|
| I | Asymptomatic | No limitation with ordinary activity | ACE-I/ARB + Beta-blocker |
| II | Mild symptoms | Limitation with strenuous activity | + Loop diuretic PRN |
| III | Moderate symptoms | Limitation with ordinary activity | + Aldosterone antagonist or ISDN/hydralazine combo |
| IV | Severe symptoms | Symptoms at rest or with minimal activity | Palliative care consideration; cardiac transplant evaluation |
Warm-Cold and Wet-Dry Classification
This classification helps categorize hemodynamic status and guides therapy:

Common Precipitants of Acute Decompensation
Remember "ADHF" — Acute Decompensated Heart Failure precipitants:
- Adherenc issues (medication or dietary nonadherence)
- Dietary indiscretion (excessive sodium or fluid intake)
- Ischemia (acute MI triggering acute failure)
- Arrhythmias (new-onset atrial fibrillation or other dysrhythmia)
- Hypertensive crisis (acute elevation in afterload)
- Renal failure (reduced diuretic efficacy, volume retention)
- Fluid overload from other sources (transfusions, IV medications)
- Infection (pneumonia, UTI, other systemic infection)
- Endocrine (thyroiditis, hyperthyroidism)
Additionally: Use of NSAIDs, cocaine, discontinuation of guideline-directed medical therapy
Diagnostic Workup
Essential labs and imaging for all decompensated HF:
| Test | Utility |
|---|---|
| CBC | Assess for anemia (may worsen HF), infection |
| CMP | Electrolytes, renal function, glucose |
| BNP or NT-proBNP | <300 pg/mL excludes HF; >900 makes HF likely; 300–900 indeterminate |
| TSH | Rule out thyroid dysfunction as reversible cause |
| EKG | Assess for ischemia, arrhythmia, chamber enlargement |
| Chest X-ray | Evaluate pulmonary edema, cardiomegaly, alternative diagnoses |
| Transthoracic echocardiogram | Assess EF, diastolic function, valve pathology, RV function |
Interpreting BNP
BNP can be falsely low in obesity and falsely elevated in CKD, females, and the elderly — always read it in clinical context.
Management by Hemodynamic Category
Universal Measures (All Patients)
- Sodium restriction: <2 grams daily
- Fluid restriction: <2 liters daily (more restrictive in severe hyponatremia)
- Daily weights: Target body weight; alert if gain >2–3 lbs in 1–2 days
- Intake/output monitoring: Document all sources
- Continue guideline-directed medical therapy if blood pressure permits
Congestion ("Wet" Status) — LMNOP Protocol
When pulmonary or peripheral edema is present, use the LMNOP mnemonic:
| Intervention | Details |
|---|---|
| Lasix (Furosemide) | Start 40–160 mg IV Q12H; typically 2.5x home oral dose. Titrate to euvolemia. |
| Morphine | 2–4 mg IV; improves dyspnea via vasodilation + anxiolysis. Use caution in hypotension/hypoxia. |
| Nitrates | Nitroglycerin IV (goal SBP >100) or isosorbide; improves preload + afterload. |
| Oxygen | Target SpO2 ≥90%; use cautiously to avoid hypercapnia in COPD overlap. |
| Position | Elevate head of bed 30–45°; improves ventilation. |
Loop diuretic equivalents (approximate for calculating doses):
| Agent | Equivalent Dose |
|---|---|
| Furosemide (Lasix) | 20 mg IV = 40 mg PO |
| Torsemide | 20 mg (more potent than furosemide) |
| Bumetanide | 1 mg (most potent, short duration) |
Loop Diuretic Conversions and When to Switch
Oral equivalence runs roughly 40 : 20 : 1 for furosemide : torsemide : bumetanide. Because furosemide's oral bioavailability is erratic (~50%) while bumetanide's is reliable (80–100%), furosemide-to-bumetanide is about 40:1 (IV or PO). Consider switching to bumetanide (or torsemide) for poor response to furosemide, diuretic resistance, or when you need a more predictable effect — bumetanide is often preferred in advanced heart failure or CKD.
Diuretic Dosing Pitfall
Do not use the same IV dose as home PO dose. IV furosemide is approximately 2.5 times more potent than oral.
Dosing and Monitoring in Acute Exacerbations
Start IV furosemide at roughly 2.5× the home oral dose. Check daily electrolytes to catch hypokalemia, hypomagnesemia, and contraction alkalosis, and monitor clinical status (daily weights, I/O, respiratory status) to know when the patient is ready to transition back to oral diuretics.
Afterload Reduction
When systolic dysfunction is present without hypotension:
- ACE inhibitor (e.g., lisinopril) or ARB (e.g., losartan)
- Hydralazine + isosorbide dinitrate combination — particularly beneficial in African Americans
- IV nitroglycerin — for acute afterload reduction
Cardiogenic Shock Management
- ICU-level care required
- Inotropic support:
- Dobutamine 2–20 mcg/kg/min (increases contractility + decreases afterload)
- Milrinone 0.25–0.75 mcg/kg/min (phosphodiesterase-3 inhibitor; inotrope + vasodilator)
- Vasopressors: Norepinephrine or dopamine if hypotensive despite inotropes
- Mechanical support: Intra-aortic balloon pump, percutaneous ventricular assist device, extracorporeal membrane oxygenation (ECMO)
- Renal replacement therapy: Consider if oliguria develops
- Urgent cardiology/transplant consultation
Documentation in the Medical Record
Every HF encounter should clearly document:
- Current NYHA functional class
- Type of HF (systolic vs. diastolic, ischemic vs. nonischemic)
- Most recent ejection fraction and date of last echocardiogram
- Dry weight (helps guide diuretic dosing on future visits)
- Current medication regimen with doses
- Renal function and electrolytes from most recent labs
- Volume status assessment (wet vs. dry)
Heart Failure Discharge Checklist
- Obtain a BNP at discharge to establish a baseline for future comparisons, and document it.
- Arrange a 7-day follow-up call (social work can help) to confirm the patient has cardiology follow-up, has obtained their medications, and is adhering to the plan.
Atrial Fibrillation: Diagnosis, Risk Stratification, and Management
Classification of Atrial Fibrillation
| Category | Duration | Clinical Notes |
|---|---|---|
| Paroxysmal | <48 hours; self-terminates | May progress to persistent AF over time |
| Persistent | >7 days; requires intervention for termination | Sustained but not permanent |
| Long-standing persistent | >1 year on anticoagulation | Chronicity increases structural remodeling |
| Permanent | Accepted by patient and provider as indefinite | Reversion not pursued |
Additionally, classify as valvular (structural valve disease or prosthetic) or nonvalvular (all other cases), as this affects anticoagulation choice.
Don't Trust the 48-Hour Window Blindly
Even when AF is presumed to be <48 hours in duration, it may actually have been present for weeks — asymptomatic the entire time — and can still cause emboli. Weigh this carefully before pursuing cardioversion without adequate anticoagulation.
Etiology of Atrial Fibrillation
Identifying the Trigger
Finding and treating the underlying cause is as important as rate/rhythm control. New AF is often provoked — infection, alcohol or stimulant use, recreational drugs, or dehydration. Ask targeted history questions and order the relevant labs and imaging to find and treat the precipitant.
Cardiac causes: - Heart failure (systolic or diastolic) - Cardiomyopathy (ischemic or nonischemic) - Myocardial infarction or active ischemia - Valvular disease (mitral stenosis particularly) - Atrial myxoma or other structural abnormality
Pulmonary causes: - COPD or other chronic lung disease - Pneumonia or acute respiratory infection - Pulmonary embolism - Obstructive sleep apnea
Metabolic/Endocrine causes: - Thyrotoxicosis or hyperthyroidism - Elevated catecholamines (pheochromocytoma)
Exogenous triggers: - Alcohol (chronic heavy use or acute binge) - Cocaine or other stimulants - Caffeine excess - Theophylline
Neurogenic causes: - Subarachnoid hemorrhage - Acute stroke - Traumatic brain injury
Acute Rate Control
When the patient is hemodynamically stable and rapid ventricular response requires rate control, use IV agents:
| Agent | IV Dosing | Mechanism | Notes |
|---|---|---|---|
| Verapamil | 5–10 mg IV bolus; may repeat in 15 min | Calcium channel blocker | Fast onset; contraindicated if hypotensive or heart failure |
| Diltiazem | 0.25 mg/kg IV bolus; repeat if needed | Calcium channel blocker | Alternative to verapamil with less negative inotropy |
| Metoprolol | 5–15 mg IV Q6H | Beta-blocker | Slower onset than IV calcium blockers |
| Esmolol | 0.5 mg/kg bolus, then infusion | Ultra-short-acting beta-blocker | Use when rapid reversibility desired |
| Digoxin | 0.5 mg IV, then 0.25 mg Q6H | Vagomimetic + AV nodal blocker | Narrow therapeutic window; less preferred acutely |
| Amiodarone | 150 mg IV over 10 min, then infusion | Antiarrhythmic (class III) | Last-line if others contraindicated or ineffective |
Maintenance Rate Control
Outpatient oral agents for rhythm control:
- Beta-blockers (metoprolol ER, atenolol, carvedilol)
- Calcium channel blockers (diltiazem ER, verapamil ER)
- Digoxin (if significant HFrEF or sedentary lifestyle)
Target heart rate depends on symptoms and function:
| Scenario | Target HR |
|---|---|
| Symptomatic AF with EF >40% | <80 bpm at rest; <110 with moderate activity |
| Asymptomatic AF with EF >40% | <110 bpm (lenient rate control) acceptable |
| AF with HFrEF (EF <40%) | <80 bpm preferred |
Stroke Risk Stratification: CHA₂DS₂-VASc Score
This score predicts stroke risk and guides anticoagulation intensity:
| Risk Factor | Points |
|---|---|
| Congestive heart failure or LV dysfunction | 1 |
| Hypertension (on treatment) | 1 |
| Age ≥75 years | 2 |
| Diabetes mellitus | 1 |
| Stroke/TIA/thromboembolism history | 2 |
| Vascular disease (MI, peripheral artery disease, aortic plaque) | 1 |
| Age 65–74 years | 1 |
| Sex category (female) | 1 |
Anticoagulation recommendations:
| Score | Recommendation |
|---|---|
| 0 (male) or 1 (female) | No anticoagulation; consider aspirin 75–325 mg daily |
| 1 (male) or 2 (female) | Anticoagulation or aspirin (shared decision-making) |
| ≥2 (male) or ≥3 (female) | Oral anticoagulation indicated |
Bleeding Risk: HAS-BLED Score
Identifies patients at higher bleeding risk while on anticoagulation:
| Risk Factor | Points |
|---|---|
| Hypertension (uncontrolled) | 1 |
| Abnormal renal/liver function | 1 |
| Stroke history | 1 |
| Bleeding history | 1 |
| Labile INR (if on warfarin) | 1 |
| Elderly (age >65) | 1 |
| Drug use (NSAIDs, antiplatelet) or alcohol excess | 1 |
Interpretation:
- Score <3: Low bleeding risk
- Score ≥3: Assess risk vs. benefit; do not withhold anticoagulation, but monitor closely
Anticoagulation Options
Anticoagulation is Essential
Most AF patients with CHA₂DS₂-VASc ≥2 require anticoagulation to reduce stroke risk by ~60%.
| Agent | Dosing | Monitoring | Key Advantages | Limitations |
|---|---|---|---|---|
| Dabigatran | 150 mg BID (110 mg BID if high bleeding risk) | No routine labs; check renal function baseline | Rapid onset/offset; predictable PK | Dyspepsia; GI bleed risk; must take intact |
| Rivaroxaban | 20 mg daily with food (15 mg if CrCl 15–30) | No routine labs; check renal function baseline | Once daily; can open capsule if needed | Food interaction; GI bleed risk |
| Apixaban | 5 mg BID (2.5 mg BID if ≥2 of: age ≥60, weight ≤60 kg, Cr ≥1.5) | No routine labs; check renal function baseline | Lowest GI bleed risk; twice-daily convenient for some | Twice-daily dosing |
| Edoxaban | 60 mg daily (30 mg if weight <60 kg, CrCl 15–50, or concurrent strong P-gp inhibitor) | No routine labs | Once daily | More strokes if CrCl >95; less data in valvular AF |
| Warfarin | Dose adjusted for INR 2–3 | INR monitoring (initially frequent, then q4 weeks) | Decades of safety data; reversible with vitamin K | Dietary interactions; narrow therapeutic window; frequent monitoring |
| Aspirin | 75–325 mg daily | No monitoring | Readily available | Inferior efficacy vs. anticoagulants; used only if AC contraindicated |
Periprocedural Anticoagulation
For an AF patient on apixaban (Eliquis) who may need surgery, plan ahead for perioperative anticoagulation and whether bridging is required. Have a plan and discuss it with your senior resident.
 Contributed by Patrick Joseph, MD
Contributed by Patrick Joseph, MD
Pulmonary Medicine Guide
Oxygen Supplementation: From Room Air to Mechanical Ventilation
Oxygen Delivery Hierarchy
Understand the spectrum of oxygen delivery systems from lowest to highest FiO2 capability:

Simple Oxygen Delivery Systems
Nasal Cannula (NC)
The most commonly used delivery system for stable patients:
FiO2 Rule of Thumb
Each liter of flow increases FiO2 by approximately 4% above room air (21%). Thus: 1 L/min = 25%, 2 L/min = 29%, 3 L/min = 33%, and so on.
- Flow rates: 1–6 L/minute
- FiO2 range: 24–44%
- Comfort: Well-tolerated; allows eating and communication
- Limitations: Cannot deliver FiO2 >44% reliably; flow >6 L/min causes nasal irritation without benefit
- Mechanism: Blends oxygen with room air at the nares
Simple Face Mask
Used when higher FiO2 needed but patient not in acute distress:
- Flow rates: 5–10 L/minute
- FiO2 range: 40–60%
- Advantages: Higher FiO2 than nasal cannula
- Disadvantages: Covers mouth; interferes with eating/speaking; patient must tolerate mask
Venturi Mask (Air-Entrainment Mask)
Delivers precise, predictable FiO2 using Bernoulli principle:
- Flow rates: 4–15 L/minute (depending on FiO2 set)
- FiO2 range: 24–50% (some models 24–60%)
- Advantage: Precise FiO2 delivery; useful in COPD where hypercapnia risk is high
- Disadvantage: Bulkier; more equipment required
Venturi setting guide:
| Color Adapter | FiO2 | Flow (L/min) |
|---|---|---|
| Blue | 24% | 3 |
| White | 28% | 4 |
| Yellow | 31% | 6 |
| Orange | 35% | 8 |
| Red | 40% | 15 |
Non-rebreather (NRB) Mask
Highest FiO2 achievable with spontaneous breathing:
- Flow rates: 10–15 L/minute (reservoir should remain ≥1/3 full)
- FiO2 range: 80–95%
- Use case: Acute hypoxemia, suspected severe hypoxia
- Mechanism: One-way valves prevent rebreathing of exhaled air; reservoir bag stores 100% oxygen
- Critical point: Ensure reservoir fills adequately with each breath; adjust flow to maintain this
High-Flow Nasal Cannula (HFNC)
Bridge between standard supplemental oxygen and non-invasive ventilation:
Physiologic Benefits
- Delivers heated, humidified oxygen at high flow rates
- Provides modest positive pressure support (PEEP approximately 3–4 cmH₂O)
- Washes out dead space, reducing rebreathing of CO₂
- Allows better nutrition and communication vs. face mask
Initial Settings and Titration
Starting parameters:
- FiO2: Start at 100%; titrate down every 15–30 minutes targeting SpO2 >90%
- Flow rate: 0.5 L/kg/min (e.g., 70 kg patient = 35 L/min)
- Can increase flow up to 2 L/kg/min if needed for distress or CO₂ retention
Titration approach:
- Begin at 100% FiO2
- If SpO2 >94%, reduce FiO2 by 10% every 15–30 min
- Adjust flow based on respiratory distress (increase if increased work of breathing)
- Monitor for improvement in respiratory rate, comfort, oxygen saturation
When HFNC Fails
Persistent hypoxemia or hypercapnia despite HFNC indicates need for escalation to non-invasive or invasive ventilation.
Non-Invasive Ventilation (NIV): BiPAP
Physiology and Indications
BiPAP (Bilevel Positive Airway Pressure) provides two levels of pressure:
- IPAP (Inspiratory Positive Airway Pressure): Applied during inspiration; supports work of breathing
- EPAP (Expiratory Positive Airway Pressure): Applied during expiration; maintains airway patency and oxygenation
Common indications: - COPD exacerbation (hypercapnic respiratory failure) - Cardiogenic pulmonary edema - Pneumonia with respiratory fatigue - Neuromuscular weakness causing hypoventilation
Initial Settings
A typical starting point for a patient in distress:
| Setting | Initial Value | Adjustment |
|---|---|---|
| IPAP | 10 cmH₂O | Increase by 2–4 cmH₂O if respiratory rate remains >30 or persistent CO₂ retention |
| EPAP | 5 cmH₂O | Increase if persistent hypoxemia or pulmonary edema; rarely >10 cmH₂O |
| FiO2 | 100% | Titrate down toward SpO2 goal |
| Backup respiratory rate | 12–16 bpm | Set slightly below patient's intrinsic rate |
Adjusting BiPAP for Clinical Response
Interpret the Problem
- Persistent high respiratory rate or CO₂ retention? → Increase IPAP to 12–16 cmH₂O
- Persistent hypoxemia? → Increase EPAP and FiO2 simultaneously
- Patient discomfort or inability to synchronize? → Lower initial pressures; increase gradually
Predictors of BiPAP Success
Strong indicators that BiPAP will be effective rather than delaying intubation:
- RR <30 at initiation (or drops below 30 within 1–2 hours)
- Tidal volume 6–8 mL/kg of ideal body weight
- Arterial pH rises ≥0.06 within first 2 hours
- PaCO₂ drops ≥8 mmHg within first 2 hours
- Patient comfort and synchronization with ventilator
Intubation Criteria
When to abandon NIV and proceed to mechanical ventilation:
| Criterion | Value |
|---|---|
| Hypercapnia | PaCO₂ >80 mmHg despite optimization |
| Severe acidemia | pH <7.25 despite BiPAP trial |
| Altered consciousness | GCS <8 (unable to protect airway) |
| Respiratory exhaustion | Severe distress, inability to cooperate |
| Acute deterioration | Decompensation during NIV trial |
COPD Exacerbation
Clinical Presentation
Acute worsening of baseline dyspnea, cough, and sputum production. Patients may also report:
- Increased sputum volume or change in character (purulent appearance suggests infection)
- Chest tightness or wheezing
- Orthopnea or worsening exercise tolerance
- Hemoptysis (suggests infection, malignancy, or PE)
Rule Out Other Causes
Acute dyspnea in a COPD patient is not always an exacerbation. Always consider pneumonia, pneumothorax, pulmonary embolism, acute coronary syndrome, and heart failure.
Initial Assessment and Diagnostics
| Test | Rationale |
|---|---|
| ABC | Assess airway patency, breathing effort, circulation |
| Chest X-ray | Identify infiltrate (pneumonia), pneumothorax, or other acute pathology |
| Arterial or venous blood gas | Assess CO₂ retention (hypercapnia), pH (acidemia), oxygenation |
| Complete blood count | Evaluate for leukocytosis (infection), anemia |
| Comprehensive metabolic panel | Renal function (affects medication clearance), electrolytes |
| Sputum culture | If purulent sputum; identify organism for antibiotic targeting |
| Procalcitonin | Adjunct to guide antibiotic initiation (elevated suggests bacterial infection) |
| ECG | Rule out acute coronary syndrome or arrhythmia |
Treatment Strategy
Bronchodilation
Rapid-acting beta-2 agonist + anticholinergic combination is the foundation:
- Albuterol 2.5 mg in 3 mL normal saline via nebulizer, delivered every 4 hours (or continuously if severe distress)
- Ipratropium 0.5 mg in 3 mL normal saline via nebulizer every 4 hours
- May combine into single nebulizer treatment for convenience
IV magnesium sulfate (2 g IV over 20 minutes) can augment bronchodilation in severe exacerbations.
Corticosteroids
Reduces airway inflammation and accelerates recovery:
- Oral prednisone 40 mg daily for 5 days (no taper necessary for short course)
- OR IV methylprednisolone 125 mg (IV methylpred ~1 mg = ~1.25 mg prednisone)
- Equivalent to approximately 100 mg IV methylprednisolone daily for 5 days
Antibiotics
Indicated if patient has one or more signs of bacterial infection:
- Purulent sputum
- Elevated temperature
- Elevated white blood cell count
- Infiltrate on chest X-ray
Antibiotic options:
| Agent | Dosing | Notes |
|---|---|---|
| Azithromycin | 500 mg daily × 3 days | Alternative day-1 loading: 500 mg then 250 mg daily × 4 more days |
| Doxycycline | 100 mg BID × 5–7 days | Avoid in renal failure; photosensitivity; good lung penetration |
| Respiratory fluoroquinolone (levofloxacin) | 750 mg daily × 5 days | Broad spectrum; good for atypical organisms; monitor QT interval |
| Amoxicillin-clavulanate | 875 mg BID × 5–7 days | If beta-lactam preferred; reasonable coverage |
Oxygen Therapy
Target SpO2: 88–92% in COPD exacerbation
Critical Concept
Many COPD patients have chronic CO₂ retention and depend on hypoxic respiratory drive. Excessive oxygen can suppress respiration and worsen hypercapnia. Monitor ABG/VBG closely and titrate conservatively.
- Start with nasal cannula 1–2 L/min
- Use Venturi mask (24–28% FiO2) if available to target precise FiO2
- Escalate to HFNC or BiPAP if inadequate response after 1–2 hours of therapy
Non-Invasive Ventilation
Consider early BiPAP if:
- Respiratory rate persistently >25
- Signs of accessory muscle use
- Hypercapnia (PaCO₂ >50) or acidemia (pH <7.35)
- Clinical deterioration despite bronchodilators and steroids
Monitoring
- Repeat blood gas at 30–60 minutes to assess response
- Reassess q1–2h initially; document respiratory rate, work of breathing, oxygen saturation
- Watch for signs requiring escalation to higher level of care (mechanical ventilation)
Pulmonary Embolism: Risk Assessment, Diagnosis, and Management
Risk Stratification
Wells Criteria for PE Probability
Clinically asymptomatic patients with low Wells score and normal D-dimer can be safely discharged without imaging:
| Clinical Finding | Points |
|---|---|
| Heart rate >100 | 1.5 |
| Clinical signs of DVT | 3 |
| PE is primary diagnosis | 3 |
| Hypoxemia (SpO₂ <90%) | 1.5 |
| Hemoptysis | 1 |
| Clinical signs of heart failure | 1.5 |
| Prior PE or DVT | 1.5 |
Score interpretation:
- ≤4 points = Low probability; D-dimer can rule out
- 4–6 points = Intermediate probability; recommend imaging
- >6 points = High probability; proceed directly to imaging
Diagnostic Workup
D-Dimer
- Highly sensitive but low specificity
- Use only in low-probability patients (Wells ≤4) to exclude PE
- Negative D-dimer essentially rules out PE
- Positive D-dimer requires imaging confirmation
Computed Tomography Pulmonary Angiography (CTPA)
The gold standard for PE diagnosis:
- Sensitivity ~95%; Specificity ~98%
- Requires iodinated contrast (avoid if contrast allergy or severe renal insufficiency)
- Risk of contrast-induced nephropathy in CKD
- Can assess RV size, RV:LV ratio (RV strain)
Ventilation-Perfusion Scan
Reserved for patients with contrast allergy or renal failure:
- High probability scan (segmental or larger perfusion defects without matched ventilation defect) = high likelihood PE
- Low probability scan = PE unlikely, can defer further testing
- Indeterminate results require additional testing
Lower Extremity Venous Ultrasound
- Detects deep vein thrombosis (DVT) as source of PE
- Can be used as initial test if DVT suspected clinically
- If proximal DVT found, treat as PE even without confirmation in pulmonary arterial tree
Echocardiography
Assess for RV strain and guide prognosis:
- RV dilation (RV:LV ratio >0.9) indicates hemodynamic impact
- RV dysfunction without hypotension suggests submassive PE
- Elevated troponin + RV strain indicates higher mortality risk
PE Risk Stratification and Treatment
Massive PE (Hemodynamically Unstable)
Presentation: Hypotension (SBP <90) or cardiogenic shock
Treatment priorities:
- Thrombolytic therapy (alteplase 15 mg bolus, then 50 mg infusion over 30 min, then 35 mg over 60 min)
- Parenteral anticoagulation (heparin drip)
- Vasopressor support if persistent hypotension
- Surgical embolectomy or catheter-directed thrombectomy if available and thrombolytics contraindicated
Time-Critical Intervention
Massive PE is immediately life-threatening. Mobilize ICU, cardiothoracic surgery, and interventional radiology.
Submassive PE (Hemodynamically Stable with RV Strain)
Presentation: Normal blood pressure but elevated troponin and/or RV dilation on echo
Treatment approach:
- Anticoagulation is primary therapy
- Thrombolytics can be considered if:
- Clinical deterioration
- Very elevated troponin/BNP
- Severe RV dysfunction
- Hemodynamic compromise develops
- Close monitoring in ICU or intermediate care
- Serial troponin and lactate to detect deterioration
Subsegmental or Low-Risk PE
Presentation: Small PE without RV strain or troponin elevation
Management:
- Anticoagulation if unprovoked or high-risk provocation
- Can observe without anticoagulation if transient provocation (surgery/immobility recently resolved)
- Outpatient follow-up and imaging surveillance may suffice
Anticoagulation and Duration
Initiation of Anticoagulation
First-line options:
| Agent | Dosing | Route | Transition |
|---|---|---|---|
| Unfractionated heparin (UFH) | 80 IU/kg bolus, then 18 IU/kg/hr infusion; adjust for aPTT 60–100 | IV | Transition to warfarin or DOAC |
| Enoxaparin (LMWH) | 1 mg/kg IV or SC Q12H; or 1.5 mg/kg SC daily | IV or SC | Transition to warfarin or DOAC |
| Fondaparinux | Weight-based SC once daily: <50 kg (5 mg), 50–100 kg (7.5 mg), >100 kg (10 mg) | SC | Transition to warfarin or DOAC |
| DOAC (rivaroxaban) | 15 mg daily × 21 days, then 20 mg daily | PO | No transition needed; continue indefinitely if unprovoked |
Long-term Anticoagulation Duration
| PE Type | Duration | Notes |
|---|---|---|
| Provoked (surgery, immobility, hospitalization) | 3–6 months | Shorter duration acceptable if transient provocation |
| Unprovoked (no clear risk factor) | ≥3 months; many continue indefinitely | Individualize based on bleeding risk and recurrence risk |
| Cancer-associated | Duration of cancer treatment + ≥3 months | Consider LMWH vs. DOAC; anticoagulate throughout chemotherapy |
| Antiphospholipid syndrome | Indefinite | High recurrence risk |
Shared Decision-Making
Discuss bleeding vs. recurrence risk with patient. After 3–6 months, reassess benefit of continuing anticoagulation.
Pleural Effusions: Classification and Management
Light's Criteria for Exudate vs. Transudate
Determining whether an effusion is exudative (pathologic) or transudative (mechanical) guides further workup:
An effusion is exudative if ONE OR MORE of the following are present:
| Criterion | Exudate Threshold |
|---|---|
| Protein ratio (pleural:serum) | >0.5 |
| LDH ratio (pleural:serum) | >0.6 |
| Absolute pleural LDH | >2/3 of upper limit of normal serum LDH |
Transudative Effusions
"Mechanical" effusions resulting from imbalance of hydrostatic and oncotic pressures:
| Cause | Pathophysiology |
|---|---|
| Congestive heart failure | Most common overall cause; elevated hydrostatic pressure |
| Cirrhosis | Ascites + portal hypertension → right heart failure |
| Nephrotic syndrome | Massive proteinuria → low serum albumin |
| Dialysis | Post-dialysis fluid shifts |
| Severe malnutrition | Reduced plasma oncotic pressure |
Management: Treat underlying condition (diuretics for CHF, lactulose for cirrhosis, etc.). Thoracentesis is diagnostic only if diagnosis uncertain.
Exudative Effusions
Pathologic processes affecting the pleura or underlying lung:
| Category | Specific Causes |
|---|---|
| Infection | Bacterial pneumonia, tuberculosis, fungal, empyema, parapneumonic |
| Malignancy | Lung, breast, lymphoma, metastatic disease; can be bloody |
| Pulmonary embolism | Often hemorrhagic; LDH elevated |
| Autoimmune | Systemic lupus erythematosus, rheumatoid arthritis, vasculitis |
| Pancreatitis | Acute pancreatitis → pancreaticpleural fistula |
| Renal failure | Uremic pleuritis |
| Post-cardiac surgery | Dressler syndrome (post-pericardiotomy syndrome) |
| Other | Esophageal rupture, aortic dissection, liver abscess |
Thoracentesis: Diagnostic and Therapeutic
Pleural fluid sampling provides diagnostic information and can provide symptomatic relief if effusion is large:
Fluids to Send and Testing
Always send pleural fluid for:
| Study | Information Obtained |
|---|---|
| Cell count and differential | WBC/RBC; neutrophil-predominant (infection/inflammation), lymphocyte-predominant (malignancy/TB), eosinophil-predominant (drug reaction, fungal) |
| Protein | Used in Light's criteria; also assessed for exudative classification |
| LDH | Used in Light's criteria for exudate determination |
| Glucose | Low glucose (<60) suggests empyema, rheumatoid pleuritis, or esophageal rupture |
| pH | pH <7.2 suggests complicated parapneumonic/empyema; pH <7.0 suggests esophageal rupture |
| Gram stain | Identifies bacteria; guides antibiotic selection |
| Bacterial culture | Grows causative organism if bacterial infection present |
| Acid-fast bacilli (AFB) culture | Diagnoses tuberculosis (low yield; still recommended) |
| Cytology | Identifies malignant cells in suspected malignancy |
Complicated Parapneumonic Effusion / Empyema
When to pursue chest tube drainage vs. antibiotics alone:
| Finding | Implication | Action |
|---|---|---|
| pH <7.2 | Loculated/walled-off infection | Chest tube or pigtail catheter needed |
| Glucose <60 | Walled-off infection | Chest tube or pigtail catheter needed |
| Positive Gram stain or culture | Documented bacteria | Chest tube or pigtail catheter needed |
| LDH >1000 | High inflammatory burden | Consider chest tube if pH/glucose also low |
| Uncomplicated parapneumonic (pH >7.2, glucose >60, negative Gram stain) | Will likely resolve with antibiotics | Antibiotics alone; recheck with imaging if inadequate response |
Hemoptysis: Evaluation and Management
Definition and Severity
Hemoptysis is expectoration of blood from the respiratory tract. Severity classification:
| Category | Volume | Urgency | Approach |
|---|---|---|---|
| Minor/mild | <30 mL per 24 hr | Outpatient workup | CXR, CT if abnormal; reassurance if normal |
| Moderate | 30–600 mL per 24 hr | Expedited workup | Same day CXR and specialist evaluation |
| Massive/life-threatening | >600 mL per 24 hr OR >100 mL/hr | EMERGENCY | ICU admission, airway protection, bronchoscopy, consider IR |
Massive Hemoptysis
Immediately place on continuous monitoring. Consider double-lumen endotracheal tube to protect airway and isolate bleeding lung. Prepare for interventional radiology or surgery.
Differential Diagnosis by Mechanism
| Mechanism | Examples |
|---|---|
| Mucosal inflammation | Acute bronchitis, upper respiratory infection, chronic bronchitis exacerbation |
| Structural airway disease | Bronchiectasis, bronchial adenoma, airway granuloma |
| Infection | Pneumonia (especially staph, fungal), lung abscess, tuberculosis |
| Malignancy | Lung cancer, metastases, lymphoma |
| Vascular causes | Pulmonary embolism, arteriovenous malformation, bleeding disorder |
| Cardiac | Acute decompensated heart failure (pink sputum), mitral stenosis |
| Vasculitis | Granulomatosis with polyangiitis, microscopic polyangiitis, Goodpasture syndrome |
Diagnostic Approach
Initial Evaluation
- History and physical exam — quantify volume, assess for fever/weight loss/risk factors
- Chest X-ray — identifies infiltrate, mass, cavitation, pneumothorax
- Complete blood count — assess hemoglobin/platelet counts
- Coagulation studies — PT, aPTT, fibrinogen if massive bleeding
- Sputum culture — if infectious cause suspected
- Sputum cytology — if malignancy suspected (low sensitivity; repeat if high clinical suspicion)
Advanced Imaging
- High-resolution CT chest — superior to CXR for detection of bronchiectasis, AVM, nodules, cavitation
- Bronchoscopy — therapeutic (tamponade, endobronchial coagulation, epinephrine instillation) and diagnostic (biopsy of lesion, specimen collection for culture); may localize source in massive hemorrhage
Interventional Radiology (IR)
- Bronchial artery angiography and embolization — definitive therapy for massive hemoptysis when bronchoscopy fails or bleeding source identified
- Success rate >90% for hemostasis
Management
Supportive Care
- NPO status until hemoptysis controlled and airway assessment complete
- IV access — 2 large-bore peripheral lines or central line in massive hemorrhage
- Type and crossmatch — have blood available if massive bleed
- Supplemental oxygen — maintain SpO2 >90%
- Monitoring — pulse oximetry, EKG, frequent vital signs
Positioning and Localization
- Position patient with bleeding lung dependent (bleeding side down)
- Bronchoscopy localizes exact site; note if left or right, what lobar/segmental distribution
Pharmacologic Therapy
| Agent | Dose | Indication | Mechanism |
|---|---|---|---|
| Epinephrine (1:1000) | 5–10 mL topically via bronchoscope | Acute hemoptysis during scope | Vasoconstriction |
| Tranexamic acid | 500 mg IV Q6H × 2–4 days | May reduce rebleeding | Antifibrinolytic |
| Aminocaproic acid | 4–5 g IV followed by 1 g/hr infusion | Alternative to tranexamic acid | Antifibrinolytic |
Endoscopic Therapy
When bronchoscopy identifies the bleeding source:
- Epinephrine injection into bleeding mucosa
- Argon plasma coagulation (APC) to cauterize visible vessel
- Cold saline irrigation to promote clot formation
- Packing or balloon tamponade (temporary) while awaiting IR intervention
Surgical Consultation
Indicated if:
- Bleeding fails to control with medical/IR therapy
- Anatomical lesion (e.g., cavitary TB) with massive recurrent hemorrhage
- Bronchiectasis confined to single lobe with refractory bleeding
Gastroenterology
Abdominal Pain: Systematic Evaluation by Location
Anatomical Approach to Chest Pain Differential
A systematic approach to location-based differential diagnosis narrows the possibilities and guides targeted workup:

Organ-Specific Differential by Location
Right Upper Quadrant (RUQ)
| Condition | Key Features | Workup |
|---|---|---|
| Acute cholecystitis | RUQ pain + fever + Murphy's sign (+) | RUQ US, elevated WBC, elevated LFTs |
| Biliary colic | RUQ/epigastric pain; fatty food trigger; no fever | RUQ US; normal labs |
| Hepatitis | RUQ pain + jaundice + malaise | LFTs (elevated transaminases), viral serology |
| Right lower lobe (RLL) pneumonia | RUQ pain + cough + fever | CXR with RLL infiltrate |
| Fitz-Hugh-Curtis | RUQ pain in young female + vaginal discharge | History of PID; laparoscopy shows perihepatitis |
Epigastric Region
| Condition | Key Features | Workup |
|---|---|---|
| Acute pancreatitis | Epigastric pain radiating to back | Elevated lipase/amylase; CT abdomen if complications |
| Peptic ulcer disease | Epigastric pain; relief with antacids; NSAID or H. pylori hx | EGD for diagnosis; H. pylori testing |
| GERD | Epigastric/substernal burning; positional; food-related | Clinical diagnosis; EGD if alarm symptoms |
| Acute MI | Epigastric discomfort with dyspnea/diaphoresis | EKG, troponin, CXR |
| Gastritis | Epigastric pain + nausea; NSAID/alcohol use | EGD; clinical diagnosis often sufficient |
Left Upper Quadrant (LUQ)
| Condition | Key Features | Workup |
|---|---|---|
| Splenic infarction | LUQ pain; sickle cell or hypercoagulable state | CT abdomen with contrast |
| Splenic rupture | LUQ pain + hemodynamic instability; trauma history | CT abdomen; surgical consultation |
| Gastritis | LUQ epigastric pain; similar to RUQ | EGD if concerning features |
| LLL pneumonia | LUQ pain + cough/fever | CXR with LLL infiltrate |
Right Lower Quadrant (RLQ)
| Condition | Key Features | Workup |
|---|---|---|
| Acute appendicitis | RLQ pain; McBurney's point tenderness; migration from periumbilicus | CT abdomen/pelvis; elevated WBC |
| Ovarian pathology | RLQ pain in female; may correlate with cycle | Pelvic US; β-hCG |
| Ectopic pregnancy | RLQ pain + vaginal bleeding in pregnant female | Serum β-hCG; pelvic US |
| Mesenteric adenitis | RLQ pain; viral prodrome; self-limited | CT may show enlarged mesenteric nodes; supportive care |
| Meckel's diverticulitis | RLQ pain (can mimic appendicitis) | Technetium scan (Meckel's scan); CT |
Left Lower Quadrant (LLQ)
| Condition | Key Features | Workup |
|---|---|---|
| Diverticulitis | LLQ pain + fever; older age; constipation history | CT abdomen/pelvis with oral/IV contrast |
| Sigmoid volvulus | LLQ pain + severe constipation; abdominal distention | Abdominal X-ray (bird's beak appearance); CT |
| Ovarian pathology | LLQ pain in female | Pelvic US; β-hCG |
| Ectopic pregnancy | LLQ pain + vaginal bleeding + pregnancy | β-hCG; pelvic US |
Diffuse Abdominal Pain
| Condition | Key Features | Workup |
|---|---|---|
| Small bowel obstruction | Diffuse colicky pain; vomiting; constipation; distention | Abdominal X-ray (air-fluid levels); CT abdomen |
| Mesenteric ischemia | Severe diffuse pain; pain out of proportion to exam | CT angiography; lactate; elevated WBC; Doppler US |
| Peritonitis | Diffuse severe pain; rigid abdomen; rebound/guarding | Imaging (look for free air); labs (elevated WBC, lactate) |
| Diabetic ketoacidosis | Abdominal pain + metabolic illness signs | Serum/urine ketones; glucose; electrolytes; ABG |
| Acute gastroenteritis | Diffuse pain + diarrhea/vomiting; prodrome | Supportive diagnosis; stool studies if bloody |
Acute Liver Failure: Recognition and Management
Definition and Etiologic Classification
Acute liver failure (ALF) is a rare syndrome of severe hepatic dysfunction developing over less than 26 weeks in a patient with previously normal liver function. Onset of coagulopathy (INR ≥1.5) without cirrhosis defines the condition.
Time-Critical Diagnosis
ALF requires urgent hospitalization in an intensive care setting with transplant capability. Contact a transplant center immediately upon suspicion.
Common Etiologies by Frequency
| Etiology | Frequency | Notes |
|---|---|---|
| Acetaminophen toxicity | 50% (US) | Most common; dose-dependent; N-acetylcysteine (NAC) very effective if given early |
| Viral hepatitis | 10–15% | HAV (fulminant in 0.1–1% of cases), HBV, HEV (high risk in pregnancy) |
| Drug-induced | 10–15% | Isoniazid, phenytoin, NSAIDs, statins, antibiotics (amoxicillin-clavulanate) |
| Autoimmune hepatitis | 5–10% | Young women; responds to steroids |
| Pregnancy-related | 1–3% | HELLP, acute fatty liver of pregnancy; worse in 3rd trimester |
| Wilson's disease | 5% (young patients) | Copper accumulation; Kayser-Fleischer rings; ceruloplasmin low |
| Budd-Chiari syndrome | 2–5% | Hepatic vein thrombosis; hypercoagulable state |
| Ischemic hepatitis | 5–15% | Severe shock/hypoxemia; rapid transaminase rise |
Fulminant Hepatic Encephalopathy
Development of hepatic encephalopathy within 8 weeks of symptom onset defines fulminant ALF and indicates worst prognosis; >80% mortality without transplant.
Initial Diagnostic Workup
Essential labs to assess severity and identify etiology:
| Test Category | Specific Tests | Interpretation |
|---|---|---|
| Synthetic function | PT/INR, albumin | INR ≥1.5 defines ALF |
| Hepatocellular injury | AST, ALT | Marked elevation (>3000) typical in ALF |
| Cholestasis | ALP, bilirubin, GGT | Assess pattern of injury; bilirubin tracks severity |
| Metabolic | CMP (glucose, electrolytes, creatinine) | Hypoglycemia, hyperammonemia, coagulopathy common |
| Renal function | BUN, creatinine, urine electrolytes | HRS (hepatorenal syndrome) develops in ~50% |
| Encephalopathy assessment | Blood ammonia, arterial blood gas | Ammonia correlates with severity; guides lactulose dosing |
| Etiologic workup | Acetaminophen level, viral serology (HAV/HBV/HCV/HEV), autoimmune markers, ceruloplasmin, imaging | See table below for specific tests by suspected etiology |
Etiology-Specific Testing
| Suspected Cause | Key Tests |
|---|---|
| Acetaminophen | Serum acetaminophen level (Rumack-Matthew nomogram for toxicity) |
| Viral hepatitis | Anti-HAV IgM, HBsAg + anti-HBc, anti-HCV (HCV RNA if positive), anti-HEV |
| Autoimmune | Anti-smooth muscle antibody (ASMA), anti-nuclear antibody (ANA), anti-liver-kidney microsomal (LKM) |
| Wilson's disease | Ceruloplasmin (low <20 mg/dL), slit-lamp exam for Kayser-Fleischer rings, 24-hr urine copper |
| Budd-Chiari | Doppler US of hepatic veins, contrast CT/MRI abdomen |
| Ischemic | Lactate, troponin, EKG, consider echocardiography |
King's College Criteria for Transplant Evaluation
Use these criteria to identify patients requiring urgent transplant evaluation:
For acetaminophen-induced ALF:
- Arterial pH <7.30, OR
- INR >6.5, OR
- Creatinine >3.4 mg/dL
For non-acetaminophen ALF:
- INR >6.5, OR
- ANY three of the following:
- Age <10 or >40 years
- Etiology: NANB hepatitis, halothane, idiosyncratic drug reaction
- Duration of jaundice >7 days before encephalopathy
- Bilirubin >17.5 mg/dL
- PT >100 seconds (INR >7)
Transplant Listing
Patients meeting King's College criteria should be urgently listed for orthotopic liver transplantation if willing and medically suitable.
Medical Management
Supportive Care Principles
- ICU admission with continuous monitoring
- Avoid all hepatotoxic medications (acetaminophen, NSAIDs, statins, etc.)
- Discontinue oral intake until mental status improves
- Total parenteral nutrition if prolonged NPO status
- Maintain glucose >100 mg/dL (hypoglycemia worsens encephalopathy)
N-Acetylcysteine (NAC) Therapy
Highly Effective in Acetaminophen Toxicity
NAC dramatically improves outcomes if given early (<24 hours), even with improvement in INR.
Standard NAC protocol:
| Phase | Dose | Route | Duration |
|---|---|---|---|
| Loading | 150 mg/kg | IV over 60 min | Single dose |
| 2nd phase | 50 mg/kg | IV over 4 hours | Single dose |
| 3rd phase | 100 mg/kg | IV over 16 hours | May repeat if INR remains elevated |
Mechanism: Replenishes hepatic glutathione stores; reduces oxidative injury
Benefit: Works best if given within 24 hours but has been shown to benefit even up to 72 hours in some cases
Management of Complications
Hepatic Encephalopathy
Mechanism: Ammonia and other neurotoxins accumulate with loss of hepatic detoxification
Treatment:
| Intervention | Mechanism | Dosing |
|---|---|---|
| Lactulose | Reduces ammonia absorption; osmotic laxative | Start 15–30 mL PO BID–TID; titrate to 2–3 soft stools daily |
| Rifaximin | Non-absorbed antibiotic; reduces ammonia-producing bacteria | 550 mg TID |
| Zinc supplementation | Cofactor for ammonia metabolism | 150–300 mg daily in divided doses |
| L-ornithine L-aspartate (LOLA) | Enhances ammonia metabolism | 10 g daily in divided doses (if available) |
| Restrict protein | Reduces nitrogen load, but must maintain adequate calories | Start at 20–30 g/day; advance as tolerated |
Avoid: Sedating medications (benzodiazepines), which worsen encephalopathy
Coagulopathy and Bleeding
- Fresh frozen plasma (FFP) — replace only before invasive procedures (does not improve outcomes)
- Vitamin K 10 mg IV daily × 3 days if deficient
- Platelets if <50 and invasive procedure planned
- Proton pump inhibitor (pantoprazole 40 mg IV BID) for stress ulcer prophylaxis
Acute Kidney Injury / Hepatorenal Syndrome
- Volume status assessment: Prerenal azotemia vs. HRS vs. acute tubular necrosis
- Supportive care: Avoid nephrotoxins
- Renal replacement therapy (RRT) if oliguria/uremia develops
Infections
- Prophylactic antibiotics often empirically given due to high infection risk
- Selective bacterial decontamination with cefotaxime or other agents
- Fungal prophylaxis (fluconazole) in high-risk patients
Cirrhosis and Portal Hypertension Complications
Severity Stratification: Child-Pugh Score
Predicts mortality and guides management urgency:
| Parameter | Points 1 | Points 2 | Points 3 |
|---|---|---|---|
| Bilirubin (mg/dL) | <2 | 2–3 | >3 |
| Albumin (g/dL) | >3.5 | 2.8–3.5 | <2.8 |
| PT prolongation (seconds) | <4 | 4–6 | >6 |
| Ascites | None | Mild | Moderate/Severe |
| Encephalopathy | None | Grade 1–2 | Grade 3–4 |
Total score interpretation:
| Score | Class | 1-Year Mortality |
|---|---|---|
| 5–6 | A | ~5% |
| 7–9 | B | ~20% |
| 10–15 | C | ~50% |
MELD Score
More objective than Child-Pugh; used for transplant listing priority:
Components:
- Bilirubin (mg/dL)
- INR (PT ratio)
- Creatinine (mg/dL)
Calculation involves logarithmic formula; use online calculator. Higher MELD = worse prognosis and higher transplant priority.
Variceal Bleeding
Acute Management
When variceal bleeding is suspected (hematemesis in cirrhotic patient):
- Two large-bore IVs and type & crossmatch
- Goal Hgb 7–9 g/dL (no over-transfusion; hypervolemia worsens portal pressure)
- Octreotide 50 mcg IV bolus, then 50 mcg/hr infusion × 48 hours
- Variceal ligation (VL) or sclerotherapy via urgent EGD (within 12 hours)
Prophylaxis for Rebleeding
After successful variceal band ligation, initiate propranolol or carvedilol to reduce portal pressure and prevent rebleeding.
Secondary Prophylaxis
After variceal bleeding, reduce rebleeding risk:
- Non-selective beta-blockers: Propranolol (titrate to heart rate reduction of 20–25%) or carvedilol 6.25–12.5 mg daily
- Repeat variceal ligation: Every 2–4 weeks until all varices obliterated
- Target: Complete variceal eradication
Spontaneous Bacterial Peritonitis (SBP)
Diagnosis
Clinical suspicion: Cirrhotic patient with ascites + fever, abdominal pain, or unexplained deterioration (encephalopathy, renal failure)
Diagnostic paracentesis:
- Send fluid for: cell count, protein, culture (preferably in blood culture bottles), glucose
- SBP diagnostic criteria: PMN count >250 cells/µL in ascitic fluid
| Finding | Typical SBP |
|---|---|
| PMN count | >250 cells/µL (diagnostic threshold) |
| Total protein | Often <1 g/dL (poor opsonic activity) |
| Glucose | May be low (<50) |
| Culture positivity | ~50% with standard technique; higher with blood culture bottles |
Treatment
Antibiotic coverage:
| Agent | Dosing | Notes |
|---|---|---|
| Ceftriaxone | 1 g IV Q12H × 5 days | First-line; excellent GI flora coverage |
| Cefotaxime | 2 g IV Q4H × 5 days | Alternative |
| Fluoroquinolone | Norfloxacin 400 mg BID × 5 days | If allergy to beta-lactams |
Albumin supplementation:
- 1.5 g/kg on day 1 (max 100 g)
- 1 g/kg on day 3 (max 100 g)
- Reduces renal failure and mortality significantly
Repeat paracentesis: At 48 hours if clinical deterioration; should show PMN reduction
SBP Prophylaxis
Indicated in cirrhotic patients with:
- Low albumin (<1.5 g/dL) AND low opsonic activity (ascitic protein <1 g/dL)
- Previous SBP (indefinite prophylaxis)
- Variceal hemorrhage (prophylactic antibiotics during acute bleed and 7 days after)
Prophylactic agents:
- Trimethoprim-sulfamethoxazole (TMP-SMX) 1 DS tablet daily
- Norfloxacin 400 mg daily (used if sulfa allergy)
Hepatic Encephalopathy Management
Precipitants
Always identify and treat underlying cause:
- Infection (SBP, UTI, pneumonia, spontaneous bacteremia)
- GI bleeding (increased nitrogen load)
- Medications (diuretics, benzodiazepines, opioids)
- Dehydration/electrolyte abnormalities
- Renal failure
- Portal vein thrombosis
- High protein intake
Treatment
First-line:
| Agent | Mechanism | Dosing |
|---|---|---|
| Lactulose | Osmotic laxative; reduces ammonia absorption | 15–30 mL BID–TID; titrate to 2–3 soft stools daily |
| Rifaximin | Non-absorbed antibiotic; inhibits ammonia-producing flora | 550 mg TID |
Second-line:
| Agent | Mechanism | Dosing |
|---|---|---|
| Zinc acetate | Cofactor for urea cycle | 220–660 mg daily in divided doses |
| L-ornithine L-aspartate | Enhances ammonia metabolism | 10 g daily (if available; used more in Europe) |
Hepatorenal Syndrome (HRS)
Definition and Types
Progressive renal failure in advanced cirrhosis without primary kidney disease. Two types:
| Type | Presentation | Prognosis |
|---|---|---|
| HRS-AKI (Type 1) | Rapid increase in Cr (>2.5 fold over 2 weeks); median survival <2 weeks without treatment | Often triggered by SBP, variceal bleed; high mortality |
| HRS-CKD (Type 2) | Gradual Cr elevation (1.5–2.5 mg/dL); associated with refractory ascites | Chronic; allows time for transplant evaluation |
Diagnostic Criteria
- Serum creatinine >1.5 mg/dL in cirrhotic patient
- No improvement after 48 hours of albumin and vasoconstrictor therapy
- Absence of parenchymal kidney disease (check urine sediment, proteinuria)
- No nephrotoxin exposure (NSAIDs, aminoglycosides)
Treatment
Involves vasoconstrictors + albumin:
| Agent | Dosing | Mechanism |
|---|---|---|
| Midodrine | 7.5–15 mg PO TID | Alpha-adrenergic agonist; systemic vasoconstriction |
| Octreotide | 100–200 mcg SQ TID | Splanchnic vasoconstriction |
| Albumin | 1 g/kg (max 100 g) on day 1; 25 g on days 2–14 | Expands plasma volume; improves renal perfusion |
| Terlipressin | 0.5–1 mg IV Q6H | Vasopressin analog (used more in Europe/Canada) |
Prognosis: HRS-AKI has poor prognosis without liver transplantation. Transplant evaluation should be urgent.
Ascites Management
Diagnostic Paracentesis
Perform to:
- Establish diagnosis of ascites etiology (SAAG, protein, cultures)
- Therapeutic benefit (remove >5 L relieves symptoms)
SAAG (serum-ascites albumin gradient):
- SAAG ≥1.1: Portal hypertension (cirrhosis, Budd-Chiari, portal vein thrombosis)
- SAAG <1.1: Non-portal hypertensive (peritoneal TB, malignancy, peritonitis)
Conservative Management
First-line for uncomplicated ascites:
- Sodium restriction to <2 g daily (most important dietary measure)
- Fluid restriction to 1.5–2 L daily if hyponatremia (<120) develops
- Daily weights to monitor fluid balance
Diuretics
If sodium restriction alone insufficient:
Spironolactone (potassium-sparing) + furosemide (loop diuretic) in combination:
| Ratio | Starting Doses | Goal | Notes |
|---|---|---|---|
| 100:40 | Spironolactone 100 mg daily + Furosemide 40 mg daily | Increase by 100 mg spiro + 40 mg furo Q3–5 days as needed | Maintains K+ balance; max spironolactone 400 mg, furosemide 160 mg daily |
Weight loss target: 0.5–1 lb daily (maintains intravascular volume)
Avoid: NSAIDs (renal failure risk); ACE-I/ARBs (hyperkalemia risk)
Refractory Ascites
Ascites refractory to sodium restriction + maximum-dose diuretics:
- Paracentesis with albumin infusion (8 g per liter removed)
- Transjugular intrahepatic portosystemic shunt (TIPS) — reduces portal pressure; complications (encephalopathy, shunt thrombosis)
- Liver transplantation — definitive therapy
Gastrointestinal Bleeding: Initial Management and Stratification
Classification and Location
Upper GI Bleeding (UGIB)
Anatomy: Bleeding proximal to the ligament of Treitz (junction of duodenum and jejunum)
| Source | Frequency | Characteristics |
|---|---|---|
| Peptic ulcer disease | 30–40% | Often H. pylori or NSAID-related |
| Esophageal varices | 15–20% | In portal hypertension; high mortality if massive |
| Mallory-Weiss tear | 5–10% | Mucosal tear from forceful vomiting/retching |
| Malignancy | 5–10% | Primary esophageal or gastric cancer |
| Portal hypertensive gastropathy | 5% | Diffuse mucosal bleeding in cirrhosis |
| Dieulafoy lesion | 1–5% | Abnormal arterial branch; high-risk for rebleeding |
| Other | 5–10% | Cameron lesions (GERD), hemobilia, aortic fistula |
Lower GI Bleeding (LGIB)
Anatomy: Bleeding distal to ligament of Treitz
| Source | Frequency | Characteristics |
|---|---|---|
| Diverticulosis | 20–30% | Often painless; colonoscopy may not identify bleeding site |
| Internal hemorrhoids | 20–30% | Bright red blood on toilet paper; visible on external exam/anoscopy |
| Angiodysplasia | 10–15% | Vascular malformations; associated with renal failure, aortic stenosis |
| Malignancy | 10–15% | Colon/rectal cancer; may have weight loss, anemia, change in bowel habits |
| Inflammatory bowel disease | 5–10% | Ulcerative colitis or Crohn's; bloody diarrhea; abdominal pain |
| Ischemic colitis | 5% | Usually left-sided; elderly with vascular risk factors |
| Other | 5–10% | Meckel's diverticulum, small bowel angiodysplasia, colitis (infectious) |
Risk Stratification
Glasgow-Blatchford Score (for UGIB)
Predicts need for intervention and mortality:
| Variable | Points |
|---|---|
| Blood pressure (SBP <100) | 1 |
| Pulse (>100) | 1 |
| Melena (presence) | 1 |
| Syncope (presence) | 2 |
| Hepatic disease (presence) | 2 |
| Cardiac failure (presence) | 2 |
| Hemoglobin (men: <100 g/L, women: <100 g/L) | 1–3 |
| Urea (>50 mg/dL) | 1 |
Score 0 = Very low risk; consider outpatient management Score ≥1 = Hospitalization recommended
AIMS65 Score
Predicts in-hospital mortality:
| Variable | Points |
|---|---|
| Age ≥65 years | 1 |
| INR ≥1.5 | 1 |
| Mental status (confusion/lethargy) | 1 |
| Shock (SBP <90 or heart rate >100 with abnormal perfusion) | 1 |
| Endoscopy findings (hematin/spurting) | 1 |
Score 0–1 = <1% mortality Score 2–3 = 5–10% mortality Score 4–5 = >20% mortality
Initial Stabilization
ABCs First
Assess airway patency, breathing adequacy, and circulation before proceeding with specific GI intervention.
Resuscitation Protocol
- Two large-bore IVs (16–18 gauge if possible) or central line if unstable
- Type & screen initially; type & crossmatch 2–4 units PRBC
- Baseline labs: CBC, CMP, PT/INR, fibrinogen, lactate
- Continuous monitoring — vital signs, SpO2, cardiac rhythm
- NPO pending endoscopy/evaluation
- Foley catheter to monitor urine output (goal >0.5 mL/kg/hr)
- Supplemental oxygen to maintain SpO2 >90%
Blood Product Transfusion Strategy
| Product | Threshold | Rationale |
|---|---|---|
| Packed RBCs | Hgb <7 g/dL | Liberal transfusion (Hgb 8–9) increases rebleeding risk in variceal bleeding |
| Fresh frozen plasma | INR >1.5 with active bleeding | Corrects coagulopathy; use only if endoscopy planned |
| Platelets | <50,000 with active bleeding | Particularly if HAS-BLED score indicates high bleeding risk |
| Cryoprecipitate | Fibrinogen <100 mg/dL | Needed if massive transfusion (>4 units PRBCs) |
Pharmacologic Therapy
Upper GI Bleeding
Proton pump inhibitor (PPI):
- High-dose IV pantoprazole 80 mg bolus, then 8 mg/hr infusion (for 72 hours)
- Reduces rebleeding risk; particularly important pre-endoscopy
For suspected variceal bleeding:
- Octreotide 50 mcg IV bolus, then 50 mcg/hr infusion × 48 hours
- Reduces splanchnic blood flow and portal pressure
- Continue regardless of endoscopic findings
Antibiotic Prophylaxis (Varices)
- Ceftriaxone 1 g IV daily (or norfloxacin 400 mg PO BID) × 7 days
- Reduces bacterial translocation and SBP risk in cirrhotic with bleeding
Endoscopic Therapy
Upper Endoscopy (EGD) Timing
- Urgent EGD (within 12 hours) for all acute UGIB unless patient not suitable for intervention
- Earlier if massive bleeding or hemodynamic instability (consider intubation for airway protection)
Endoscopic interventions by bleeding source:
| Source | Technique | Success |
|---|---|---|
| Peptic ulcer | Epinephrine injection ± cautery ± clip placement | ~90% |
| Varices | Endoscopic variceal ligation (VL) or sclerotherapy | ~90%; VL superior for rebleeding prevention |
| Mallory-Weiss | Cautery, injection, or clip; usually self-limited | ~80% |
| Dieulafoy | Injection, cautery, clip, or endoscopic band | ~95% |
Lower Colonoscopy
- Colonoscopy within 24 hours for nonmassive LGIB to identify source
- During active bleeding: Direct injection, thermal coagulation, or clip placement
- Angiodysplasia: Thermal coagulation or argon plasma coagulation (APC)
- Diverticular bleeding: Usually no intervention needed (hemostasis achieved endoscopically if actively bleeding)
Small Bowel Evaluation
If UGIB and LGIB workups unrevealing, consider video capsule endoscopy or double-balloon enteroscopy for small bowel source.
Intervention Escalation
Rebleeding Despite Endoscopy
- Repeat endoscopy — success decreases with each attempt
- Interventional radiology: Angiography with arterial embolization
- Surgical evaluation — if persistent bleeding uncontrolled by endoscopy/IR
Acute Pancreatitis: Diagnosis and Management
Definition and Etiologic Spectrum
Acute pancreatitis is inflammation of the pancreas with sudden onset of epigastric pain. Two leading causes account for ~80% of cases: biliary obstruction and alcohol.
Common Etiologies
| Category | Causes |
|---|---|
| Gallstone-related | Biliary obstruction; highest-risk if stone <5 mm (passage into CBD) |
| Alcohol | Acute intoxication or chronic heavy use; dose-related |
| Drug-induced | L-asparaginase, azathioprine, sulfonamides, pentamidine, didanosine, valproate, steroids, diuretics, sulfonamides |
| Metabolic | Hypertriglyceridemia (>1000 mg/dL), hypercalcemia, hypothermia |
| Infectious | Mumps, Coxsackie B, Mycoplasma (rare in developed countries) |
| Structural | Pancreatic cancer, PCP, sphincter of Oddi dysfunction |
| Idiopathic | ~20% of cases; diagnosis of exclusion |
Memory aid: "GET SMASHED"
- Gallstones, Ethanol
- Trauma, Tumor, Toxins
- Steroid use, Sphincter of Oddi dysfunction, Superbug (infection)
- Metabolic (HTG, hypercalcemia)
- Autoimmune
- SED (smoking-related?)
- Hyperlipidemia, Hypertriglyceridemia
- END (endoscopy-related), Ethanol
- Drugs, Deficiency (nutritional)
Diagnostic Criteria
Diagnosis requires TWO of THREE:
- Characteristic abdominal pain: Epigastric, radiating to back, gradual onset (hours), peak at 6–12 hours
- Elevated pancreatic enzymes:
- Amylase >3× upper limit normal (more nonspecific; rises/falls within days)
- Lipase >3× upper limit normal (more specific; elevated longer than amylase)
- Characteristic imaging findings: CT abdomen (pancreatic edema, necrosis, peripancreatic fat stranding)
Lipase Preferred
Lipase is more specific and sensitive than amylase for pancreatitis and remains elevated longer (up to 14 days vs. 3–5 days for amylase).
Prognostic Scoring
Ranson's Criteria
Predicts mortality and complications:
| At Admission | At 48 Hours |
|---|---|
| Age >55 years | Hematocrit drop >10% |
| WBC >16,000/µL | BUN rise >5 mg/dL |
| Glucose >200 mg/dL | Serum calcium <8 mg/dL |
| LDH >350 IU/L | Alb drop >1 g/dL |
| AST >250 IU/L | PaO2 <60 mmHg |
Score interpretation:
| Score | Mortality |
|---|---|
| <3 | <1% |
| 3–4 | 15–20% |
| 5–6 | 30–40% |
| >6 | >50% |
BISAP Score
Simpler; calculated at admission:
| Variable | Points |
|---|---|
| BUN >25 mg/dL | 1 |
| Impaired mental status | 1 |
| SIRS (≥2 criteria) | 1 |
| Age >60 years | 1 |
| Pleural effusion | 1 |
Score 0–2 = <2% mortality Score ≥3 = Increased mortality and complications
Workup and Imaging
Initial labs:
- Amylase, lipase — diagnosing pancreatitis
- Comprehensive metabolic panel — glucose (may rise), electrolytes, renal function, calcium
- Liver enzymes, bilirubin — if biliary pancreatitis suspected
- Triglycerides, cholesterol — if metabolic cause suspected
- Albumin, lactate — assess severity
- CBC — baseline Hgb/Hct for transfusion triggers
Imaging:
| Test | Indication | Findings |
|---|---|---|
| Abdominal ultrasound (RUQ focus) | Rule out gallstones; assess for CBD dilation | Stones, wall thickening, pericholecystic fluid |
| CT abdomen/pelvis with contrast | If not improving by 48–72 hours OR severe pancreatitis | Pancreatic edema, fat stranding (interstitial edema), pancreatic necrosis (20–30% of cases), fluid collections |
| MRCP | Suspected CBD obstruction or cholangitis | Direct visualization of biliary tree; therapeutic ERCP can be performed |
Management Strategy
Supportive Care (Universal)
The foundation of treatment; most mild pancreatitis resolves with supportive care:
- NPO status initially; advance diet as tolerated (see below)
- Aggressive fluid resuscitation:
- Lactated Ringer's preferred (normal saline associated with hyperchloremic acidosis)
- Goal: Urine output 0.5–1 mL/kg/hr; may require 150–300 mL/hr initially
- Continue fluids until clinical improvement (reduced pain, oral intake tolerated)
- Pain control:
- IV opioids (morphine, hydromorphone)
- Avoid IM injections (risk of abscess/loculation)
- Meperidine less preferred (spasms sphincter of Oddi)
- Prophylactic measures:
- No role for antibiotics in uncomplicated, mild pancreatitis
- PPIs if PUD risk factors
Diet Advancement
Start oral intake as soon as tolerated (goal: within 24 hours if possible):
- Mild pancreatitis: Advance to regular diet as tolerated; no specific diet restriction needed
- Severe pancreatitis: Start with clear liquid diet; advance slowly if tolerating
- If unable to eat: Consider enteral nutrition (nasogastric feeding) — improves outcomes vs. total parenteral nutrition
Specific Therapy by Etiology
Biliary pancreatitis with cholangitis: Urgent ERCP with sphincterotomy
Alcohol-related: Nutritional support; thiamine; folate; magnesium replacement
Diverticulitis: Uncomplicated vs. Complicated
Definition and Pathophysiology
Diverticulitis is inflammation of one or more colonic diverticula (outpouchings through the muscular wall). Inflammation can be uncomplicated (simple inflammation) or complicated (perforation, abscess, fistula).
Epidemiology
Incidence increases with age (rare <50 years in US, higher prevalence in Western countries with low-fiber diets). Right-sided diverticulitis more common in Asia.
Clinical Presentation and Diagnosis
Typical Presentation
- LLQ pain (RLQ if right colon involved)
- Fever (variable; may be absent in mild disease)
- Altered bowel habits (constipation or loose stools)
- Nausea/vomiting (if complicated)
Diagnostic Imaging
CT abdomen/pelvis with IV and oral contrast is gold standard:
| Finding | Interpretation |
|---|---|
| Colonic wall thickening (>5 mm) | Indicative of colitis |
| Diverticula with surrounding inflammation | Diagnostic of diverticulitis |
| Pericolic fat stranding | Indicates degree of inflammation |
| Localized abscess | Suggests complicated disease; may require drainage |
| Free air | Suggests perforation; consider surgical consultation |
| Fistula tract | Communication with bladder (colovesical), small bowel (coloenteric), or other organ |
Laboratory findings:
- Elevated WBC (may be normal in mild disease)
- Elevated CRP/procalcitonin
- No pathognomonic lab tests
Uncomplicated Diverticulitis
Definition: Simple inflammation without abscess, perforation, or fistula
Outpatient Management (Select Patients)
Can manage at home if:
- Immunocompetent
- Tolerating oral intake
- No signs of sepsis
- Reliable follow-up
- Pain well-controlled
Prescribe:
- Bowel rest (clear liquid diet)
- Oral antibiotics covering gram-negative and anaerobes:
- Cipro 500 mg BID + metronidazole 500 mg TID × 7–10 days, OR
- Amoxicillin-clavulanate 875 mg BID × 7–10 days
- (Can defer antibiotics in mild, uncomplicated disease if no fever/elevated WBC)
- Analgesia (acetaminophen preferred; avoid NSAIDs if possible due to increased perforation risk)
- Follow-up: Call or visit in 24–48 hours; if worsening, go to ED
Hospitalization Indications
- Fever >102°F or signs of sepsis
- Inability to tolerate oral intake
- Immunocompromised (diabetes, immunosuppression, age >50 with comorbidities)
- Intractable pain
- Failed outpatient therapy (symptoms worsening after 48–72 hours of oral antibiotics)
- First episode in some centers (controversial; if uncomplicated, outpatient is reasonable)
Inpatient protocol:
- NPO
- IV fluid resuscitation
- IV antibiotics: Ceftriaxone 1 g IV Q12H + metronidazole 500 mg IV Q8H (or piperacillin-tazobactam 4.5 g IV Q6H)
- Advance diet as tolerated (usually within 48–72 hours if improving)
Complicated Diverticulitis
Diverticulitis with Abscess
CT findings: Localized fluid collection with enhanced rim
Management:
- IR-guided percutaneous drainage if abscess >4 cm
- IV antibiotics
- Delayed elective colectomy (6–8 weeks after resolution) to prevent recurrence
Diverticulitis with Perforation and Peritonitis
Presentation: Severe pain, rigid abdomen, signs of peritonitis
CT findings: Free air, free fluid, wide pericolic stranding
Management:
- Immediate surgical consultation
- NPO, IV fluids, broad-spectrum antibiotics
- Operative intervention: Primary resection with anastomosis (if patient stable and proximal adequate) vs. Hartmann procedure (resection with colostomy) if unstable
Diverticulitis with Fistula
Colovesical fistula (colon-bladder communication; most common):
- Presentation: Pneumaturia, fecaluria, recurrent UTIs
- Diagnosis: CT with fecal material in bladder, barium enema showing fistula tract
- Management: Elective surgical resection of affected bowel segment
Coloenteric or colouterine fistulas: Similar principles; surgical consultation for timing and approach
Biliary Tract Disease: From Colic to Cholangitis
Spectrum of Acute Biliary Illness
Understanding the progression from simple gallstones to life-threatening cholangitis guides urgency of intervention:

Biliary Colic
Presentation
- Sudden RUQ or epigastric pain lasting 30 minutes to several hours
- No fever (distinguishes from cholecystitis)
- No peritonitis (no Murphy's sign)
- Often triggered by fatty meal
Workup
| Test | Finding |
|---|---|
| RUQ ultrasound | Gallstones present; normal GB wall and no pericholecystic fluid |
| Labs | Normal; WBC normal, LFTs normal |
Management
- Conservative management; stone will typically pass
- Elective cholecystectomy if recurrent symptoms (prevents progression to cholecystitis)
Acute Cholecystitis
Presentation
- RUQ pain >6 hours (prolonged compared to biliary colic)
- Fever (present in ~70% of cases)
- Murphy's sign positive (inspiratory arrest during RUQ palpation with deep breath)
- Elevated WBC
Diagnostic Criteria
Tokyo Guidelines for Acute Cholecystitis Diagnosis:
Definite: 1 + 1 from below:
- RUQ tenderness + fever or elevated inflammatory markers
- Imaging findings:
- Gallstones + pericholecystic edema/fluid OR
- Wall thickening (>4 mm) + pericholecystic fluid OR
- Sonographic Murphy's sign
Imaging
| Modality | Finding |
|---|---|
| RUQ US (first-line) | Gallstones + pericholecystic fluid; positive Murphy's sign; GB wall thickening |
| CT abdomen | Increased GB wall enhancement; pericholecystic stranding; useful if complications suspected |
| HIDA scan | Nonvisualization of GB (cystic duct obstruction); used if ultrasound nondiagnostic |
Management
- NPO
- IV fluids and electrolyte correction
- IV antibiotics: Cefotaxime 2 g IV Q4H + metronidazole 500 mg IV Q8H (covers gram-negative + anaerobes)
- Analgesia: IV opioids
- Definitive: Cholecystectomy (laparoscopic preferred) within 24–48 hours of diagnosis
- Early cholecystectomy (within 72 hours) reduces complications and length of stay
- Percutaneous cholecystostomy if patient too ill for surgery (bridge to definitive treatment)
Common Bile Duct Obstruction / Choledocholithiasis
Presentation
- Jaundice (scleral icterus, dark urine)
- Abdominal pain (epigastric or RUQ)
- Elevated conjugated bilirubin and alkaline phosphatase
- May be asymptomatic (discovered incidentally on imaging)
Diagnosis
| Modality | Use |
|---|---|
| RUQ ultrasound | Dilated CBD (>6 mm), may show stone |
| MRCP | Gold standard for imaging CBD; can visualize stones, strictures, masses |
| ERCP | Therapeutic: stone extraction via sphincterotomy |
Management
Uncomplicated choledocholithiasis:
- ERCP with endoscopic sphincterotomy + stone extraction (success >90%)
- Followed by cholecystectomy if symptomatic GB disease
Mirizzi syndrome (external CBD compression by impacted stone):
- ERCP with stone extraction (relief of compression)
- Cholecystectomy
Acute Cholangitis (Charcot's Triad)
Clinical Presentation
Charcot's triad (present in only ~50% of cases):
- Fever (>38.5°C)
- Right upper quadrant pain
- Jaundice
Mortality increases with Reynolds' pentad (adds):
- Altered mental status
- Hypotension
Medical Emergency
Acute cholangitis is a medical/surgical emergency with mortality ~5–10% if untreated, higher if septic shock develops.
Pathophysiology
Bacterial infection of obstructed biliary system. Obstruction (stone, stricture, malignancy) + bacteria (often gram-negative or anaerobes from intestine) + stasis = infection.
Diagnostic Workup
| Test | Finding |
|---|---|
| Labs | Elevated bilirubin, elevated ALP/GGT, elevated transaminases, elevated WBC, elevated lactate (if septic) |
| Blood cultures | Positive in 50–80% (draw before antibiotics) |
| RUQ ultrasound | Dilated intrahepatic/extrahepatic bile ducts; may show stone or mass |
| MRCP | Definitive; shows obstruction site and cause |
Management (URGENT)
- Immediate broad-spectrum IV antibiotics:
- Cefotaxime 2 g IV Q4H (or cefepime/ciprofloxacin if cephalosporin allergy)
- + Metronidazole 500 mg IV Q8H (anaerobic coverage)
-
± Vancomycin if immunocompromised or recent hospital exposure (MRSA risk)
-
IV fluid resuscitation — may have sepsis; target urine output 0.5–1 mL/kg/hr
-
Urgent ERCP with endoscopic sphincterotomy (within 24 hours, sooner if septic or unstable):
- Extract stone(s) or relieve obstruction
- Success rate >90%
- If ERCP fails: percutaneous transhepatic cholangiography (PTC) or surgical intervention
Do Not Delay
Do NOT delay ERCP to await imaging confirmation if clinical suspicion is high and patient deteriorating.
Diarrhea: Classification, Evaluation, and Management
Temporal Classification
Duration-based classification guides workup strategy:
| Category | Duration | Typical Causes |
|---|---|---|
| Acute | <14 days | Viral (norovirus, rotavirus), bacterial (Salmonella, Shigella, E. coli, Campylobacter), toxins, medications |
| Persistent | 14–30 days | Protozoal (Giardia, Entamoeba), bacterial overgrowth, IBD (early presentation), bile acid malabsorption |
| Chronic | >30 days | IBD (UC, Crohn's), IBS, malabsorption, medication effect (PPIs, antibiotics), functional causes |
Pathophysiologic Classification
Understanding the mechanism guides diagnostic testing:
Osmotic Diarrhea
Mechanism: Unabsorbed osmotically active substances in bowel lumen
Characteristics: - Improves with fasting - Stool osmotic gap >125 mOsm/kg - Examples: Lactose intolerance, magnesium-containing laxatives, polyol malabsorption
Secretory Diarrhea
Mechanism: Active ion secretion exceeds absorption
Characteristics: - Persists with fasting (distinguishes from osmotic) - Stool osmotic gap <125 mOsm/kg - High stool output (often >1 L/day) - Examples: Cholera, VIP-secreting tumor, bile acid malabsorption, certain medications (SSRIs)
Inflammatory Diarrhea
Mechanism: Mucosal inflammation → exudation + increased motility
Characteristics: - Blood/mucus in stool - Fever, abdominal pain - Elevated fecal calprotectin/lactoferrin - Examples: IBD (UC, Crohn's), infectious colitis (C. difficile, Salmonella), ischemic colitis
Motility-Related Diarrhea
Mechanism: Abnormal colonic motility
Characteristics: - Often small-volume, frequent stools - Often associated with abdominal pain/cramping - Examples: IBS, diabetic neuropathy, scleroderma
Acute Diarrhea Workup
Most acute diarrhea is viral and self-limited; selective testing indicated:
| Indication | Test |
|---|---|
| Bloody stool or fever | Stool culture (Salmonella, Shigella, Campylobacter, STEC O157:H7) |
| Abdominal pain + fever >38.5°C | Fecal leukocytes or lactoferrin (suggests inflammatory); stool culture |
| Recent antibiotics | C. difficile toxin/GDH (if diarrhea onset during or within 10 days of antibiotic) |
| Immunocompromised (HIV CD4 <200) | Ova & parasites, stool culture, consideration of special stains |
| Bloody diarrhea + thrombocytopenia | Stool culture for STEC; consider HUS; no antimotility agents |
First-line supportive care:
- Oral rehydration solution (glucose-electrolyte solutions; WHO formulation preferred)
- Antimotility agents contraindicated if fever/bloody stool (risk of toxic megacolon/HUS)
- Antidiarrheals (loperamide, diphenoxylate) safe in nonbloody, afebrile diarrhea
Chronic Diarrhea Workup
Initial approach:
- History: Onset, duration, stool frequency, presence of blood/mucus, timing (nocturnal vs. daytime), relation to food/stress
- Physical exam: Signs of dehydration, weight loss, abdominal examination
- Labs: CBC, CMP (electrolytes, renal function), thyroid function, tissue transglutaminase (celiac screening)
- Imaging: Consider CT abdomen if weight loss or alarm symptoms
Further testing guided by classification:
- Stool osmolality, electrolytes (osmotic gap calculation)
- Fecal fat (72-hour collection to assess for steatorrhea)
- Fecal calprotectin/lactoferrin (screen for IBD/inflammatory causes)
- Colonoscopy (if alarm features, bloody stool, age >50, family history of colorectal cancer)
Clostridioides difficile Infection (CDI)
Epidemiology and Risk Factors
Risk factors:
- Antibiotic use (fluoroquinolones, clindamycin, cephalosporins; risk increases with duration)
- Advanced age
- Severe underlying illness
- Immunosuppression
- Prior CDI
- PPI use (reduces gastric acid barrier)
Clinical Presentation
Spectrum ranges from asymptomatic colonization to fulminant colitis:
- Mild-moderate: Watery diarrhea (≥3 unformed stools/24 hr), abdominal cramping, low-grade fever
- Fulminant: Toxic megacolon, sepsis, shock, high mortality
Diagnosis
NAAT (nucleic acid amplification test) or enzyme immunoassay (EIA) for C. difficile toxins A/B:
Testing Pitfalls
Do NOT retest during treatment or for 4 weeks after treatment ends (test of cure not recommended; toxin can persist).
Treatment
First-line therapy:
| Severity | Agent | Dosing | Duration |
|---|---|---|---|
| Initial, non-severe | Vancomycin (oral only; doesn't get absorbed systemically) | 125 mg PO QID | 10 days |
| Severe (Cr >1.5× baseline or fever/leukocytosis) | Vancomycin | 125 mg PO QID | 10 days |
| Fulminant | Vancomycin | 500 mg PO/NG QID + IV metronidazole 500 mg Q8H | 10 days |
| Recurrent (first or second) | Fidaxomicin | 200 mg PO BID | 10 days |
Second-line agents:
- Fidaxomicin 200 mg BID × 10 days (superior for preventing recurrence vs. vancomycin; higher cost)
- Metronidazole (only if vancomycin unavailable; inferior outcomes for non-severe CDI)
Adjunctive measures:
- Discontinue offending antibiotic if possible
- Avoid antimotility agents (risk of toxic megacolon)
- Fecal microbiota transplantation (FMT) for multiple recurrences
Renal Medicine Survival Guide
Acute Kidney Injury
Acute kidney injury (AKI) represents a rapid decline in kidney function, classified by the KDIGO staging system based on changes in serum creatinine and urine output.
KDIGO Staging
| Stage | Creatinine Change | Urine Output | Clinical Significance |
|---|---|---|---|
| 1 | 1.5-1.9× baseline OR ≥0.3 absolute increase | <0.5 mL/kg/h × 6-12 hours | Mild elevation, immediate evaluation needed |
| 2 | 2-2.9× baseline | <0.5 mL/kg/h × ≥12 hours | Moderate decline, intervention indicated |
| 3 | ≥3× baseline OR ≥4.0 absolute increase OR RRT initiated | <0.3 mL/kg/h × ≥24 hours OR anuria ≥12 hours | Severe, often requires renal replacement therapy |
Pathophysiology and Differential Diagnosis
Pre-renal AKI
Caused by inadequate renal perfusion from volume depletion, hypotension, or reduced effective circulating volume.
Common Etiologies: - Hypovolemia (GI losses, diuretics, hemorrhage) - Hypotension (sepsis, cardiogenic shock) - Decreased effective circulating volume (heart failure, cirrhosis, nephrotic syndrome)
Urinary Findings: - Fractional excretion of sodium (FeNa) <1% - BUN:creatinine ratio >20 - Urine sodium <20 mEq/L - Urine osmolality >500 mOsm/kg
Intrinsic Renal AKI
Direct kidney tissue injury from acute tubular necrosis (ATN), acute interstitial nephritis (AIN), or glomerulonephritis.
ATN (Ischemic or Nephrotoxic): - FeNa >2% - Muddy brown casts on urinalysis - Often irreversible if prolonged
AIN (Drug-Induced or Infection-Related): - WBC casts with eosinophiluria - Common offenders: NSAIDs, beta-lactams, sulfonamides, proton pump inhibitors - Rash and fever may accompany
Glomerulonephritis: - RBC casts on microscopy - Hematuria and proteinuria - May have systemic symptoms
Post-renal AKI
Obstruction to urine flow distal to the kidney, amenable to intervention.
Common Causes: - Benign prostatic hyperplasia (BPH) - Kidney stones - Malignancy - Urinary catheter obstruction
Key Finding: Hydronephrosis on renal ultrasound
Diagnostic Approach
Initial Workup
Obtain basic metabolic panel (BMP), urinalysis with microscopy, urine electrolytes for FeNa calculation, and renal ultrasound. Consider renal biopsy only if diagnosis remains unclear after non-invasive evaluation.
Essential Tests: - Serum creatinine (baseline and current) - BUN - Electrolytes (particularly potassium) - Urinalysis with microscopy - Urine electrolytes (sodium, osmolality) - Renal ultrasound to assess hydronephrosis and kidney size
Management Principles
Critical First Steps
Immediately identify and treat the underlying cause. Discontinue all nephrotoxic medications and address volume status appropriately.
General Approach:
- Identify etiology - Pre-renal vs intrinsic vs post-renal
- Stop nephrotoxins - ACE inhibitors, ARBs, NSAIDs, aminoglycosides
- Volume management - Aggressive fluid resuscitation for pre-renal; fluid restriction for intrinsic with oliguria
- Relieve obstruction - Percutaneous nephrostomy or foley placement for post-renal causes
- Supportive care - Control electrolytes, acid-base status, and fluid balance
Indications for Emergent Dialysis (AEIOU Mnemonic)
| Indication | Details | Time Frame |
|---|---|---|
| Acidosis | Severe metabolic acidosis unresponsive to medical therapy (usually pH <7.1) | Emergent |
| Electrolyte | Severe hyperkalemia refractory to medical management (K+ >6.5 with ECG changes) | Emergent |
| Ingestion | Toxic ingestions amenable to dialysis (methanol, ethylene glycol, salicylates) | Varies |
| Overload | Pulmonary edema unresponsive to diuretics | Urgent |
| Uremia | Uremic encephalopathy, pericarditis, or severe symptoms | Urgent |
Chronic Kidney Disease
Chronic kidney disease (CKD) is defined as reduced glomerular filtration rate (GFR) or kidney damage persisting for ≥3 months, staged by GFR.
CKD Stages
| Stage | GFR (mL/min/1.73m²) | Description | Kidney Function |
|---|---|---|---|
| G1 | ≥90 | Normal or high | Normal with kidney disease |
| G2 | 60-89 | Mildly decreased | Normal or mildly decreased |
| G3a | 45-59 | Mildly to moderately decreased | Mild-moderate decline |
| G3b | 30-44 | Moderately to severely decreased | Moderate-severe decline |
| G4 | 15-29 | Severely decreased | Severe decline, prepare for RRT |
| G5 | <15 OR on dialysis | Kidney failure | Requires RRT |
Complications of Chronic Kidney Disease
Monitor for Complications
CKD patients develop multiple metabolic and hematologic complications that require proactive management to prevent morbidity and mortality.
- Anemia - From erythropoietin deficiency; contribute to fatigue and cardiac strain
- Mineral and bone disease - Hyperphosphatemia, hypocalcemia, secondary hyperparathyroidism leading to bone loss and vascular calcification
- Metabolic acidosis - Accumulation of organic and inorganic acids
- Hyperkalemia - Impaired renal excretion of potassium
- Volume overload - Sodium and fluid retention, contributing to hypertension and pulmonary edema
- Uremic toxins - Accumulation causes uremic syndrome with neurologic and gastrointestinal manifestations
Management Strategy
Key Interventions
Blood pressure control and glycemic control form the foundation of CKD management. ACE inhibitors and ARBs provide cardio-renal protection beyond blood pressure lowering.
Pharmacologic Approach: - Blood pressure control - Target <120 mmHg; use ACE inhibitors or ARBs as first-line for proteinuria reduction - Glycemic control - Strict control in diabetes (HbA1c 7-8%) - Phosphate binders - Start when phosphate rises (calcium acetate, sevelamer, lanthanum) - Vitamin D supplementation - Calcitriol as GFR falls - Erythropoiesis-stimulating agents - For hemoglobin 10-12 g/dL (avoid targets >12) - Avoid nephrotoxins - NSAIDs, contrast, certain antibiotics
Diuretic Therapy
Diuretics are essential for managing volume overload in kidney disease, heart failure, and cirrhosis. Understanding their mechanism and escalation strategy optimizes outcomes.
Diuresis Escalation Algorithm
Follow this stepwise approach when initial diuretic therapy proves inadequate:

Diuretic Equivalency
Understanding equipotent doses ensures appropriate escalation:
| Agent | Equivalent Dose | Route Notes |
|---|---|---|
| Furosemide (Lasix) | 40 mg PO = 20 mg IV | Standard reference |
| Torsemide | 20 mg | 4× more potent than furosemide |
| Bumetanide | 1 mg | 40× more potent than furosemide |
Dosing Strategy
When escalating therapy, remember that 2.5× the patient's home dose is often needed to achieve initial diuresis. IV dosing is typically 40-50% of equivalent oral dose.
Adverse Effects by Diuretic Class
| Adverse Effect | Loop Diuretics | Thiazide Diuretics | K-Sparing Diuretics |
|---|---|---|---|
| Electrolyte abnormalities | ↓ Na, K, Mg | ↓ Na, K, Mg | ↑ K, ↑ H+ |
| Metabolic | ↑ Uric acid (gout) | ↑ Glucose, ↑ Lipids | Metabolic acidosis |
| Endocrine | — | Hyperglycemia | — |
| Other | Ototoxicity (high doses) | Pancreatitis, photosensitivity | Gynecomastia (spironolactone) |
Special Population Dosing
Adjust Strategy by Comorbidity
Different disease states require modified diuretic approaches to prevent complications.
Heart Failure: - Increase frequency before increasing dose - May require BID IV dosing - Combine with dietary sodium restriction
Nephrotic Syndrome: - Use 2-3× standard doses - Diuresis is often limited by low serum albumin - Consider IV albumin before diuretic in select cases
Cirrhosis: - Use spironolactone:furosemide ratio of 2.5:1 to prevent hypokalemia - Target weight loss ≤0.5 kg/day to avoid acute renal failure - Higher doses of spironolactone needed to block aldosterone
IV Furosemide Dosing Strategy
Use this formula to estimate appropriate initial IV dose in patients with reduced renal function:
$$\text{Initial IV Lasix dose (mg)} = 30 \times \text{Creatinine (mg/dL)}$$
Then titrate based on response, doubling dose every 2-4 hours if needed.
Intravenous Fluid Composition and Management
Selection of appropriate IV fluids is critical for resuscitation and maintenance therapy. Understanding electrolyte content and osmolality guides clinical decision-making.
IV Fluid Electrolyte Composition
| Solution | Na⁺ (mEq/L) | K⁺ (mEq/L) | Cl⁻ (mEq/L) | HCO₃⁻ (mEq/L) | Glucose (g/L) | Osmolality (mOsm/L) |
|---|---|---|---|---|---|---|
| D5W | 0 | 0 | 0 | 0 | 50 | 253 |
| Half-normal saline (½NS) | 77 | 0 | 77 | 0 | 0 | 154 |
| Normal saline (NS) | 154 | 0 | 154 | 0 | 0 | 308 |
| Lactated Ringer's (LR) | 130 | 4 | 109 | 28 | 0 | 275 |
| 3% hypertonic saline | 513 | 0 | 513 | 0 | 0 | 1026 |
| Normal plasma | 135-145 | 3.5-5 | 100-110 | 22-26 | 80-100 | 280-295 |
Classification of IV Solutions
By Tonicity Relative to Plasma:
- Hypotonic (osmolality <280) - D5W, ½NS; distribute to intracellular space; useful for hypernatremia but risk of cerebral edema
- Isotonic (osmolality 270-310) - NS, LR; remain in extracellular space; first-line for resuscitation
- Hypertonic (osmolality >310) - 3% NaCl; pulls fluid from intracellular to extracellular space; reserved for symptomatic hypernatremia or cerebral edema
By Composition:
- Crystalloids - Small electrolytes and glucose; cheap, rapid distribution, large volumes needed
- Colloids - Large molecules (albumin, dextran, hetastarch); expensive, stay intravascular longer, controversial efficacy in sepsis
Maintenance Fluid Calculations
Holliday-Segar Formula (pediatric and applicable to adults):
$$\text{First 10 kg} = 4 \text{ mL/kg/hour}$$ $$\text{Next 10 kg} = 2 \text{ mL/kg/hour}$$ $$\text{Remaining weight} = 1 \text{ mL/kg/hour}$$
Simplified Adult Formula:
$$\text{Maintenance rate (mL/hr)} = \text{Weight (kg)} + 40$$
Calculation Example
A 70 kg patient requires: 70 + 40 = 110 mL/hr maintenance fluid (approximately 2.6 L/day)
Third-Spacing Concept
Third spacing refers to accumulation of fluid in non-functional spaces (interstitium) that is unavailable for perfusion:
- Ascites - Portal hypertension increases Starling forces
- Burn injuries - Increased capillary permeability from inflammation
- Bowel obstruction - Fluid sequestration in bowel wall and lumen
- Peritonitis - Inflammatory response causes interstitial edema
Clinical Implication
Patients with third spacing may appear to have adequate intravascular volume on exam while being profoundly intravascularly depleted. Aggressive fluid resuscitation may be necessary despite peripheral edema or ascites.
Management Strategy: - Recognize third-spacing and compensate with additional IV fluids - Monitor for overload (pulmonary edema, peripheral edema) while ensuring adequate perfusion - Reassess volume status frequently, especially in critically ill patients
Infectious Disease Survival Guide
Evaluation of Fever
Fever is a regulated increase in body temperature, distinct from unregulated hyperthermia. Understanding the underlying etiology is essential for appropriate management.
Fever Pathophysiology Categories
Environmental/Thermoregulatory Failure: - Heat stroke - Excessive environmental heat overwhelming dissipation mechanisms - Malignant hyperthermia - Genetic predisposition triggered by certain anesthetics - Neuroleptic malignant syndrome (NMS) - Dopamine antagonist-induced rigidity and hyperthermia - Serotonin syndrome - Excessive serotonergic activity from drug interactions
Inflammation-Mediated Fever: - Infection (bacterial, viral, fungal) - Thromboembolic phenomena (myocardial infarction, pulmonary embolism) - Autoimmune conditions (rheumatoid arthritis, systemic lupus erythematosus) - Malignancy (lymphoma, renal cell carcinoma) - Medication reactions
Diagnostic Approach
Clinical Assessment
Begin by characterizing the fever pattern. A detailed history of exposures, travel, sick contacts, and medication changes guides the differential diagnosis.
Key History Elements: - Duration of fever and temperature pattern (constant vs intermittent) - Associated systemic symptoms (chills, night sweats, weight loss) - Recent travel and endemic exposures - Sick contacts and epidemiologic risk factors - Medication history (especially antibiotics, anticonvulsants) - Recent procedures or interventions
Physical Examination: - Obtain full vital signs including accurate temperature - Comprehensive physical exam for localizing signs - Look for rashes, lymphadenopathy, hepatosplenomegaly - Cardiac exam for murmurs (endocarditis)
Fever of Unknown Origin (FUO)
FUO is classically defined as fever documented on multiple occasions during ≥3 weeks of illness without an established diagnosis after at least one week of investigation.
Classic FUO Etiologies (in order of frequency):
| Category | Common Diagnoses | Frequency |
|---|---|---|
| Infection | Tuberculosis, endocarditis, abscess, osteomyelitis | ~30% |
| Malignancy | Lymphoma, leukemia, renal cell carcinoma | ~20% |
| Rheumatologic | Systemic lupus erythematosus, vasculitis, adult Still's disease | ~15% |
| Other | Granulomatous colitis, drug fever, pulmonary embolism | ~20% |
| Unknown | No diagnosis despite thorough evaluation | ~15% |
Investigation Strategy:
Avoid Unnecessary Antibiotics
Do not empirically treat FUO with antibiotics. Comprehensive workup must precede treatment to avoid masking diagnosis and selecting resistant organisms.
- Laboratory: CBC with differential, comprehensive metabolic panel, liver function tests, inflammatory markers (ESR, CRP), blood cultures (multiple sets before antibiotics)
- Imaging: Chest X-ray, abdominal ultrasound or CT, consider PET scan if diagnosis remains elusive
- Specific testing: TB testing (PPD, IGRA), serologies (EBV, CMV, toxoplasma, brucella depending on exposure), ECG and echocardiography if endocarditis suspected
- Medication review: Discontinue unnecessary medications; "drug fever" resolves within 48-72 hours of cessation
Neutropenic Fever
Neutropenic fever is a medical emergency defined as a single temperature ≥38.3°C or ≥38°C sustained for ≥1 hour with absolute neutrophil count <500.
Risk Stratification: - High-risk: Prolonged neutropenia (>7 days expected), unstable vital signs, signs of organ dysfunction - Low-risk: Brief neutropenia, stable, no comorbidities
Empiric Antibiotic Algorithm:

Key Principles: - Obtain cultures before any antibiotics - Avoid delays - empiric broad-spectrum coverage within 1 hour - Reassess at 48-72 hours; de-escalate if cultures identify organism - Continue until ANC recovery, not just clinical improvement
Fever in Returned Traveler
Fever developing in a traveler or in the weeks after travel requires consideration of endemic pathogens. Geographic region is paramount.
| Geographic Region | Most Common Etiologies | Less Common But Important |
|---|---|---|
| Sub-Saharan Africa | Malaria, typhoid, dengue | Sleeping sickness, typhus, Q fever |
| Southeast Asia | Dengue, malaria, typhoid | Chikungunya, typhus, leptospirosis |
| Central America | Dengue, malaria | Enteric fever, chagas disease |
| South America | Dengue, malaria, enteric fever | Yellow fever, chagas disease, bartonellosis |
| Caribbean | Dengue, chikungunya | Malaria (limited areas) |
| South Asia | Typhoid, dengue, malaria | Enteric fever, chikungunya |
| Middle East | Enteric fever, brucellosis | Q fever, leishmaniasis |
Diagnostic Approach
Always ask specifically about the geographic region and time since return. Malaria can present up to a year after exposure. Blood smear or rapid antigen testing should be obtained early given the potentially fatal consequences of delayed diagnosis.
Sepsis and Septic Shock
Sepsis represents the body's dysregulated response to infection, characterized by systemic inflammation and organ dysfunction.
Definition and Diagnostic Criteria
SIRS Criteria (≥2 required; retained by CMS): - Temperature >38°C or <36°C - Heart rate >90 bpm - Respiratory rate >20/min or PaCO₂ <32 mmHg - WBC count >12,000 or <4,000 cells/mm³
Sepsis = SIRS criteria + documented or presumed infection
Septic Shock = Sepsis + hypotension unresponsive to 30 mL/kg crystalloid OR need for vasopressors to maintain MAP ≥65 mmHg
SOFA Score for Risk Stratification
The SOFA (Sequential Organ Failure Assessment) score quantifies organ dysfunction and predicts mortality.
| System | Score 0 | Score 1 | Score 2 | Score 3 | Score 4 |
|---|---|---|---|---|---|
| Respiratory | PaO₂/FiO₂ ≥400 | PaO₂/FiO₂ <400 | PaO₂/FiO₂ <300 | PaO₂/FiO₂ <200 (on MV) | PaO₂/FiO₂ <100 (on MV) |
| Coagulation | Platelets ≥150 | 100-149 | 50-99 | 20-49 | <20 |
| Liver | Bili <1.2 | 1.2-1.9 | 2-5.9 | 6-11.9 | >11.9 |
| Cardiovascular | MAP ≥70 | MAP <70 | Dopamine <5 or dobutamine | Dopamine 5-15 or epi <0.1 | Dopamine >15 or epi >0.1 |
| Renal | Cr <1.2 | Cr 1.2-1.9 | Cr 2-3.5 | Cr 3.6-5 | Cr >5 |
| Neuro | GCS 15 | 13-14 | 10-12 | 6-9 | <6 |
Mortality Risk
Each point increase in SOFA score correlates with increasing mortality risk. SOFA ≥2 in the setting of infection has mortality approaching 10%; SOFA ≥3 approaches 50% mortality.
qSOFA Score
The quick SOFA (qSOFA) identifies high-risk patients at bedside using three variables:
| Variable | Criterion |
|---|---|
| Respiratory rate | ≥22 breaths/min |
| Altered mental status | Any confusion or decreased consciousness |
| Systolic blood pressure | ≤100 mmHg |
Interpretation: ≥2 qSOFA points indicates high risk for adverse outcome and warrants aggressive intervention.
Initial Diagnostic Workup
Time-Sensitive Interventions
Every hour of delay in appropriate antibiotics increases mortality. Obtain cultures before antibiotics but do not delay treatment for cultures.
Laboratory Studies: - Complete blood count with differential - Comprehensive metabolic panel (assess organ function) - Prothrombin time (PT/INR) - Lactate level (marker of tissue hypoperfusion) - Blood cultures - minimum 2 sets before antibiotics - Arterial or venous blood gas - Procalcitonin (markers of bacterial infection; not diagnostic alone)
Source Identification: - Chest X-ray (pneumonia, acute respiratory distress) - Urinalysis and urine culture - Wound cultures if open wound - Consider abdominal imaging if intra-abdominal source suspected
Lactic Acidosis in Sepsis
Lactate accumulates from tissue hypoperfusion and impaired hepatic metabolism:
| Type | Mechanism | Clinical Context | Prognosis |
|---|---|---|---|
| Type A (Hypoxic) | Tissue hypoxia and anaerobic metabolism | Septic shock, cardiogenic shock, hypovolemic shock | Worse; indicates severe tissue hypoperfusion |
| Type B (Non-hypoxic) | Toxin-mediated, impaired clearance, or metabolism | Liver disease, malignancy, medications (nucleoside reverse transcriptase inhibitors) | Variable; depends on underlying cause |
Early Goal-Directed Therapy (EGDT)
Aggressive early intervention in the first 3 hours improves sepsis outcomes:

Key Interventions: - Fluid: Balanced crystalloid (normal saline, Lactated Ringer's) 30 mL/kg for hypotension or lactate ≥4 - Vasopressors (if MAP remains <65 mmHg after fluids): Norepinephrine 0.01-2 μg/kg/min + vasopressin 0.04 units/min (not titrated) as first-line - Source control: Drainage of abscess, removal of infected device, operative debridement as needed - Reassess lactate: 2-3 hours after initial resuscitation; persistent elevation indicates ongoing hypoperfusion
Empiric Antibiotic Selection by Source
| Infection Source | First-Line Regimen | Alternative | Duration |
|---|---|---|---|
| Critical illness/urosepsis | Ceftriaxone 1-2g q12h + azithromycin 500mg daily OR respiratory fluoroquinolone (levofloxacin 750mg daily) | Vancomycin if penicillin allergy | 5-7 days |
| Healthcare-associated pneumonia | Antipseudomonal: piperacillin-tazobactam 4.5g q6h or meropenem 1g q8h + MRSA coverage if risk factors | Add fluoroquinolone for coverage expansion | 7-10 days |
| Community-acquired pneumonia | Ceftriaxone 1g q12h + azithromycin 500mg daily OR respiratory fluoroquinolone | Amoxicillin-clavulanate if outpatient | 5-7 days |
| Uncomplicated UTI | Ceftriaxone 1-2g q12h | Fluoroquinolone, TMP-SMX | 7 days |
| Skin/soft tissue | Vancomycin 15-20mg/kg q12h + piperacillin-tazobactam 4.5g q6h + clindamycin 600mg q8h | Beta-lactam/beta-lactamase inhibitor monotherapy if not severe | 7-14 days |
| Intra-abdominal (peritonitis, cholecystitis) | Piperacillin-tazobactam 4.5g q6h OR meropenem 1g q8h | Add fluoroquinolone for additional coverage | 7-10 days |
De-escalation: - At 48-72 hours, review culture results and adjust to narrowest appropriate spectrum - Transition to oral antibiotics when clinical improvement and GI tolerance established - Discontinue vasopressors when hemodynamically stable
Pneumonia
Pneumonia classification and empiric antibiotic selection depend on patient risk factors and epidemiologic context.
Pneumonia Classification and Microbiology
| Classification | Risk Factors | Common Organisms | Mortality |
|---|---|---|---|
| CAP | Healthy outpatient | Streptococcus pneumoniae, Haemophilus influenzae, Mycoplasma, Legionella, viruses | 1-5% |
| HAP | Hospitalization >48 hrs, no mechanical ventilation | Gram-negatives (Pseudomonas, Klebsiella), MRSA, anaerobes | 20-30% |
| VAP | Mechanical ventilation >48 hrs | Pseudomonas, MRSA, Acinetobacter, Enterobacteriaceae | 25-50% |
| Aspiration PNA | Loss of airway protection (swallow dysfunction, decreased LOC) | Anaerobes, microaerophilic streptococci, gram-negatives | Variable |
CURB-65 and Pneumonia Severity Index
CURB-65 Score (≥2 predicts severe disease): - Confusion (acute mental status change) - Urea >7 mmol/L - Respiratory rate ≥30 - Blood pressure (SBP ≤100 or DBP ≤60) - 65+ years old
Pneumonia Severity Index (PSI) Classes for Disposition:
| Class | CURB-65 | Clinical Features | Disposition | Mortality |
|---|---|---|---|---|
| I | 0 | Age <50, no comorbidities | Outpatient | <1% |
| II | 1 | Mild-moderate CAP | Brief hospitalization | 1-2% |
| III | — | Moderate CAP | Hospital admission | 2-3% |
| IV | — | Severe features | Hospital admission | 8-15% |
| V | — | Very severe features | ICU admission | >30% |
Severe Community-Acquired Pneumonia Criteria
Severe CAP requires ICU admission and intensive management:
Major Criteria (one sufficient): - Septic shock requiring vasopressors - Respiratory failure requiring mechanical ventilation
Minor Criteria (≥3 needed for "severe"): - Respiratory rate ≥30 breaths/min - Partial pressure of oxygen <60 mmHg - Multilobar opacities on imaging - Core body temperature <36°C - Encephalopathy - Uremia (BUN >7 mmol/L or Cr ≥1.5 mg/dL) - WBC <4 × 10³/L - Platelets <100 × 10³/L
Pneumonia Treatment Guidelines
| Pneumonia Type | Empiric Regimen | Duration | Notes |
|---|---|---|---|
| CAP (outpatient) | Amoxicillin-clavulanate OR macrolide OR respiratory fluoroquinolone | 5-7 days | Macrolide alone insufficient for most patients |
| CAP (hospitalized) | Ceftriaxone 1g q12h + azithromycin 500mg daily OR respiratory fluoroquinolone | 5-7 days | Add vancomycin if risk for MRSA |
| Severe CAP | Add vancomycin to ceftriaxone + azithromycin regimen | 7-10 days | Consider pseudomonal coverage if risk factors |
| HAP/VAP | Piperacillin-tazobactam OR carbapenem (meropenem, imipenem) + consider MRSA coverage | 7-10 days | Avoid aminoglycosides as monotherapy |
| Aspiration PNA | Piperacillin-tazobactam OR ampicillin-sulbactam | 7-10 days | Anaerobic coverage essential if abscess/empyema |
| PCP (HIV+, CD4 <200) | TMP-SMX (high-dose) IV or PO | 21 days | Add corticosteroids if PaO₂ <70 or A-a gradient >35 |
De-escalation Strategy
Do not continue broad-spectrum empiric regimens once cultures identify organism and antibiotic sensitivities are known. Narrow spectrum to reduce resistance selection and adverse effects.
Urinary Tract Infections
UTIs range from asymptomatic bacteriuria to life-threatening urosepsis. Treatment decisions depend on complexity and symptoms.
Uncomplicated vs Complicated UTI
Uncomplicated UTI: - Non-pregnant women with acute cystitis or pyelonephritis - No structural or neurologic urinary tract abnormalities - Normal renal function
Complicated UTI: - Pregnant women (risk of hematogenous spread) - Men (longer urethra, risk of prostatitis) - Urinary catheters or stents - Structural abnormalities (obstruction, reflux, neurogenic bladder) - Renal impairment - Immunosuppression
Common Uropathogens
| Organism | Uncomplicated Cystitis | Pyelonephritis | Catheterized Patients | Nosocomial UTI |
|---|---|---|---|---|
| E. coli | ++ | ++ | + | + |
| K. pneumoniae | + | + | ++ | ++ |
| P. aeruginosa | — | — | ++ | ++ |
| Enterococcus | — | — | ++ | + |
| S. saprophyticus | ++ | — | — | — |
UTI Treatment by Type
| Diagnosis | Empiric Therapy | Duration | Alternative |
|---|---|---|---|
| Asymptomatic bacteriuria | No treatment (except pregnant women) | — | Pregnant: cephalexin or nitrofurantoin 7 days |
| Acute cystitis (uncomplicated) | Nitrofurantoin 100mg BID OR TMP-SMX DS BID OR fosfomycin 3g single dose | 3-5 days | Avoid fluoroquinolones for uncomplicated disease |
| Acute pyelonephritis (outpatient) | Fluoroquinolone (levofloxacin 750mg daily) OR TMP-SMX DS BID | 7-14 days | Ceftriaxone if unable to tolerate PO |
| Acute pyelonephritis (inpatient) | Ceftriaxone 1-2g q12h OR fluoroquinolone IV OR piperacillin-tazobactam | 10-14 days | Transition to PO after defervescence |
| Urethritis (NGU/chlamydia) | Ceftriaxone 250mg IM single dose + doxycycline 100mg BID | 7 days (doxy) | Azithromycin 1g × 1 if doxycycline contraindicated |
| Prostatitis (acute) | Fluoroquinolone (ciprofloxacin, levofloxacin) | 10-14 days | TMP-SMX DS BID as alternative |
| Prostatitis (chronic) | Fluoroquinolone OR TMP-SMX | 6-12 weeks | Requires prolonged therapy for tissue penetration |
| Renal abscess | IV antibiotics (cephalosporin, fluoroquinolone, or carbapenem) + percutaneous drainage | 4-6 weeks | Nephrectomy if drainage unsuccessful |
Avoid Catheter-Induced Delays
Do not treat asymptomatic catheter-associated bacteriuria unless symptomatic or patient is pregnant. Catheter replacement without antimicrobials is preferred management.
Skin and Soft Tissue Infections
Bacterial skin infections range from minor impetigo to life-threatening necrotizing fasciitis. Rapid recognition and appropriate therapy are essential.
Definitions and Epidemiology
| Entity | Definition | Typical Organism | Key Features |
|---|---|---|---|
| Impetigo | Superficial skin infection in stratum corneum | Group A Streptococcus, S. aureus | Honey-crusted lesions, highly contagious |
| Erysipelas | Infection of superficial dermis with lymphatic involvement | Group A Streptococcus | Sharply demarcated, raised, often facial |
| Cellulitis | Non-suppurative deeper dermal and subcutaneous infection | Streptococci (GAS, GBS), S. aureus | Spreading erythema, warmth, edema |
| Necrotizing fasciitis (NF) | Rapidly spreading deep tissue infection with high mortality | Polymicrobial (Type I) or monomicrobial (Type II) | Systemic toxicity out of proportion to exam |
| Gas gangrene | Myonecrosis from gas-producing organisms | Clostridium perfringens | Severe pain, crepitus, shock |
| Osteomyelitis | Bone infection, hematogenous or contiguous | S. aureus most common | Localized pain, swelling, fever (may be absent) |
Special Exposures and Organisms
| Exposure/Bite | Key Organisms | Notable Agents |
|---|---|---|
| Cat bite | Pasteurella multocida (50-80%) | Aggressive infection risk |
| Dog bite | Pasteurella, Staphylococcus, Streptococcus | Lower infection rate than cat bites |
| Human bite | Eikenella, Staphylococcus, Streptococcus | High polymicrobial infection risk |
| Seawater exposure | Vibrio vulnificus, Vibrio parahaemolyticus | Aggressive, often with bacteremia |
| Fresh water | Aeromonas, Vibrio | Risk with open wounds |
Necrotizing Fasciitis: A Clinical Emergency
NF requires immediate recognition and surgical intervention. Mortality approaches 30% even with treatment.
Clinical Red Flags
Systemic toxicity (shock, delirium) out of proportion to cutaneous findings is the hallmark of NF. Severe pain beyond the area of visible erythema is another warning sign. These patients require immediate surgical consultation.
Type I (Polymicrobial ~70% of cases): - Typically follows abdominal surgery or perforation - Mixed gram-positive, gram-negative, and anaerobic organisms - Often includes anaerobes
Type II (Monomicrobial ~25% of cases): - Group A Streptococcus ± Staphylococcus aureus - Often follows minor trauma or surgery - Rapid progression
Type III (Monomicrobial ~5% of cases): - Gram-negative organisms - IV drug use-related - Marine-associated (Vibrio)
Surgical Urgency: Do not delay for imaging. Clinical suspicion warrants immediate surgical exploration.
Osteomyelitis Classification and Management
| Type | Pathogenesis | Common Organisms | Imaging | Treatment |
|---|---|---|---|---|
| Hematogenous | Bacteremia seeding bone | S. aureus, Streptococci | MRI most sensitive | 4-6 weeks IV ABx |
| Contiguous | Direct inoculation (trauma, surgery) | S. aureus, gram-negatives, anaerobes | X-ray, CT | 4-6 weeks IV ABx + surgical debridement |
| Vascular insufficiency | Compromised blood flow (diabetes) | Gram-negatives, anaerobes, polymicrobial | Plain films, vascular assessment | Extended oral ABx + wound care |
Special Population - Sickle Cell Disease: - Organisms: Salmonella (atypical for non-sickle patients) - Mechanism: Splenic infarction impairs opsonization and complement activation
Cellulitis Treatment Approach
Non-Purulent Cellulitis (no collection present): - Ceftriaxone 1-2g q12h IV OR cefazolin 1-2g q8h IV - Or cephalexin 500mg QID PO for mild cases
Purulent Cellulitis (collection present - drain first, then antibiotics): - TMP-SMX DS BID × 7 days OR - Doxycycline 100mg BID × 7 days OR - Vancomycin for severe disease
Necrotizing Fasciitis: - Surgical debridement FIRST (may require multiple operations) - Vancomycin 15-20mg/kg q12h + - Piperacillin-tazobactam 4.5g q6h OR - Penicillin G 4 million units q4h + clindamycin 600mg q8h (for streptococcal anaerobic coverage)
Meningitis
Bacterial meningitis is a medical emergency with mortality approaching 20% even with treatment. Recognition and empiric therapy within the first hour dramatically improve outcomes.
Clinical Presentation
Classic meningitis triad occurs in only 50% of patients: - Fever - Headache (severe) - Neck stiffness (meningismus)
Additional findings: - Photophobia - Altered mental status or confusion - Kernig's sign (pain with knee extension when hip flexed) - Brudzinski's sign (neck flexion causes hip/knee flexion) - Petechial or purpuric rash (characteristic of meningococcemia)
Etiologies by Age and Risk
| Age Group | Primary Organisms | Secondary Organisms |
|---|---|---|
| Neonates (0-3mo) | Group B Streptococcus, E. coli (K1), Listeria monocytogenes | Gram-negatives |
| Children (3mo-18yr) | Neisseria meningitidis, Streptococcus pneumoniae | H. influenzae (if unvaccinated) |
| Adults (18-50yr) | N. meningitidis, S. pneumoniae | Gram-negatives |
| Elderly (>50yr) | S. pneumoniae, Listeria monocytogenes, Gram-negatives | N. meningitidis |
| Immunocompromised | Listeria, Cryptococcus, Gram-negatives | Mycobacteria |
Meningococcemia
Neisseria meningitidis bacteremia often presents with petechial or purpuric rash. Watch for fulminant sepsis (meningococcal septic shock). Young patients with rash + fever warrant empiric meningitis coverage immediately.
Diagnostic Approach and CSF Findings
Before Lumbar Puncture (LP): - Obtain blood cultures immediately (before antibiotics) - CT head if: focal neurologic deficit, papilledema, immunosuppression, age >60, signs of increased ICP - Do NOT delay antibiotics for imaging or LP
Cerebrospinal Fluid (CSF) Analysis:
| Parameter | Normal | Bacterial | Tuberculous | Fungal | Viral |
|---|---|---|---|---|---|
| Appearance | Clear | Turbid/purulent | Clear/turbid | Clear/turbid | Clear |
| Opening Pressure | 10-20 cm H₂O | 20-100+ | 20-100+ | 20-100 | 15-40 |
| WBC count | <5 | 100-26,000 | 10-500 | 10-500 | 10-1,000 |
| WBC predominant | — | PMN | Lymphocytes | Lymphocytes | Lymphocytes |
| Glucose | 40-70 | <40 (CSF:blood <0.4) | <40 | <40 | >40 (CSF:blood >0.5) |
| Protein | <45 | 100-500 | 100-500 | 100-500 | 50-100 |
| Gram stain | Negative | 60-90% sensitive | Negative | Negative | Negative |
| Culture | Negative | 70-80% (pre-ABx) | 10-80% | 10-50% | Negative |
Empiric Treatment
Do Not Delay Treatment
If meningitis is suspected clinically, initiate antibiotics immediately, even before lumbar puncture or imaging. Delay in antibiotics increases mortality.

Empiric Antibiotic Regimens:
| Patient Population | Regimen | Notes |
|---|---|---|
| Age 18-50 (meningitis coverage) | Ceftriaxone 2g IV q12h + Vancomycin 15-20mg/kg IV q12h | Add ampicillin if age >50 or immunocompromised |
| Age >50 OR immunocompromised | Ceftriaxone 2g IV q12h + Vancomycin 15-20mg/kg IV q12h + Ampicillin 2g IV q4h | Ampicillin covers Listeria |
| Severe penicillin allergy | Fluoroquinolone (moxifloxacin) + Vancomycin | Chloramphenicol if not available |
Additional Therapies: - Dexamethasone: 10mg IV q6h × 4 days (initiated with first antibiotic dose reduces mortality) - Adjunctive agents: Vancomycin levels should be 15-20 μg/mL; ensure adequate penetration into CSF
Viral Meningitis (HSV Suspected): - Acyclovir 10mg/kg IV q8h × 7-14 days - Continue until HSV and VZV excluded by PCR
Fungal Meningitis (Cryptococcal in immunocompromised): - Amphotericin B 0.7-1 mg/kg/day IV + Fluconazole 400-800mg daily × 8-10 weeks
HIV and Opportunistic Infections
Opportunistic infections (OIs) are the primary driver of morbidity and mortality in advanced HIV. Prophylaxis and treatment regimens depend on CD4 count and immune reconstitution.
Opportunistic Infection Prophylaxis by CD4 Count
| CD4 Count | Primary Prophylaxis | Additional | Duration |
|---|---|---|---|
| <200 | TMP-SMX DS daily (also covers Toxo + PCP) | — | Until CD4 >200 × 3 months on ART |
| <100 | Continue TMP-SMX | Add azithromycin 1200mg weekly (MAC prophylaxis) | Until CD4 >100 × 3 months |
| <50 | Continue above | Add itraconazole 200mg daily (fungal prophylaxis) | Until CD4 >50 × 3 months |
| >200 | Discontinue PCP prophylaxis | Consider discontinuing others if CD4 sustained | Monitor for immune reconstitution |
Opportunistic Infection Treatment
Tuberculosis (TB-HIV co-infection): - Standard TB regimen: INH + rifampin + pyrazinamide + ethambutol - Dosing adjusted in HIV due to drug interactions - ART initiation timing depends on CD4 (earlier if CD4 <50)
Pneumocystis Pneumonia (PCP): - First-line: TMP-SMX (15-20mg/kg/day TMP component) × 21 days - Alternative: Dapsone + trimethoprim or atovaquone - Add corticosteroids if PaO₂ <70 or A-a gradient >35
Toxoplasma Encephalitis: - Pyrimethamine 200mg load then 50-100mg daily + - Sulfadiazine 1-1.5g q6h × - Folinic acid (leucovorin) 10-20mg daily for bone marrow protection - Duration: minimum 6 weeks, often until immune reconstitution
Cryptococcal Meningitis: - Induction: Amphotericin B 0.7-1 mg/kg/day IV + fluconazole 400-800mg daily - Consolidation: Fluconazole 400mg daily × 8 weeks - Maintenance: Fluconazole 200mg daily (long-term suppression)
Cytomegalovirus (CMV): - CMV retinitis: Ganciclovir IV 5mg/kg q12h or foscarnet - CMV esophagitis/colitis: Ganciclovir or foscarnet
Candidiasis: - Oropharyngeal: Fluconazole 200-400mg daily × 7-14 days - Esophageal: Fluconazole 400-800mg daily × 14-21 days - Disseminated: Fluconazole or amphotericin B
Immune Reconstitution Inflammatory Syndrome (IRIS)
Rapid CD4 recovery on ART may cause paradoxical worsening of OI symptoms as immune system reactivates against pathogens. Monitor closely in first weeks of ART initiation, especially with CD4 <50.
Endocrinology
Diabetic Ketoacidosis
Diabetic ketoacidosis (DKA) is a life-threatening hyperglycemic emergency characterized by severe metabolic acidosis, elevated anion gap, and ketonemia. Early recognition and aggressive management are essential.
Precipitating Factors (The "I"s)
- Insulin noncompliance - Most common precipitant in known diabetics
- Infection - Pneumonia, urinary tract infection, sepsis
- Inflammation - Pancreatitis, myocarditis, gastroenteritis
- Ischemia - Myocardial infarction, stroke, mesenteric ischemia
- Intoxication - Alcohol, cocaine, other substances
- Iatrogenic - Corticosteroids, antipsychotics, SGLT2 inhibitors
- Trauma - Motor vehicle collision, fall, burn injury
Clinical Presentation
Rapid Onset
DKA symptoms may develop over hours. Classic presentation includes polyuria, polydipsia, nausea/vomiting, and progressive altered mental status.
Symptoms: - Polyuria and polydipsia (osmotic effect of hyperglycemia) - Nausea and vomiting (from acidosis and ketonemia) - Abdominal pain (may mimic acute abdomen) - Dyspnea and Kussmaul's respirations (compensatory for metabolic acidosis) - Altered mental status progressing to coma
Physical Examination: - Signs of dehydration (tachycardia, hypotension, poor skin turgor) - Kussmaul's respirations - deep, rapid breathing with fruity odor - Altered mental status or frank coma - Abdominal tenderness (may be present despite benign imaging)
Laboratory Findings
Pseudohyponatremia
Severe hyperglycemia causes water shifts from intracellular to extracellular space, decreasing measured serum sodium. Calculate corrected sodium: Corrected Na = Measured Na + [2.4 × (Glucose - 100)/100]
Expected Laboratory Pattern:
| Test | Finding | Explanation |
|---|---|---|
| Glucose | >250 mg/dL | Severe hyperglycemia |
| pH | <7.35 | Metabolic acidosis |
| Bicarbonate | <15 mEq/L | Consumed by buffering acid |
| Anion gap | >12 | Elevated from ketoacids (acetoacetate, beta-hydroxybutyrate) |
| Potassium | Often elevated | Acidosis drives K+ out of cells despite total body depletion |
| BUN/Creatinine | Elevated | Dehydration concentrates urine |
| Osmolality | >320 mOsm/kg | Markedly elevated from glucose and electrolytes |
| Urinalysis | Positive ketones | Ketonuria from accelerated lipolysis |
DKA vs Hyperosmolar Hyperglycemic State (HHS)
| Feature | DKA | HHS |
|---|---|---|
| Glucose | Usually 250-600 | Often >600 |
| Serum osmolality | <320 | >320 |
| Arterial pH | <7.35 | >7.35 |
| Bicarbonate | <15 | >15 |
| Anion gap | Elevated | Normal |
| Ketones | Present | Absent/minimal |
| Mental status | Variable | More altered |
| Mortality | 1-5% | 5-15% |
Initial Diagnostic Workup
Urgent Laboratory Studies: - Comprehensive metabolic panel (electrolytes, glucose, BUN, creatinine) - Arterial or venous blood gas (assess pH and bicarbonate) - Serum ketones or beta-hydroxybutyrate (more specific than urine ketones) - Urinalysis with ketones - Complete blood count (assess for infection as precipitant) - Venous or arterial lactate - Pregnancy test (if female of childbearing age) - Magnesium level (depletions common)
Assess for Precipitants: - Blood cultures if infection suspected - Chest X-ray - Electrocardiogram (rule out MI as precipitant) - Abdominal imaging if abdominal pain prominent - Urine drug screen if intoxication possible
DKA Management Algorithm

Critical Management Points
Potassium Paradox
Despite total body potassium depletion, initial serum potassium is often elevated due to acidosis. As insulin and fluids are given, potassium will fall dramatically. Monitor closely and supplement proactively to avoid hypokalemia-induced arrhythmias.
Fluid Resuscitation: - Start aggressive crystalloid replacement: 1-2L in first 1-2 hours - Route electrolytes based on corrected sodium - After initial bolus: 250-500 mL/hr based on sodium level - When glucose <250: switch to D5-containing solution (prevents hypoglycemia) - Target restoration of circulating volume, which dramatically improves glucose clearance
Insulin Therapy: - Initial bolus: 10 units regular IV (optional; some protocols omit) - Continuous infusion: 0.1 U/kg/hour (e.g., 70 kg patient = 7 U/hr) - Goal: decrease blood glucose 75-100 mg/dL per hour - As anion gap closes (usually 8-12 hours), transition to subcutaneous insulin - Critical: Do NOT stop IV insulin immediately; overlap with subcutaneous
Potassium Management: - If K+ >5: monitor, no replacement - If K+ 3.5-5: add 10-20 mEq/hour to IV fluids - If K+ <3.5: HOLD insulin immediately, give aggressive potassium (PO + IV) - Check level q2-4h initially, then q4-6h as situation stabilizes
Bicarbonate: - Rarely indicated; avoid unless pH <6.9 - If given: 100 mmol sodium bicarbonate in 200 mL sterile water at 200 mL/hour - May worsen hypokalemia and hypomagnesemia - Repeat only if pH remains <7.0 after 2 hours
Monitoring: - BMP every 4 hours until patient stable - Point-of-care glucose checks every 1-2 hours - Continuous cardiac monitor (especially for potassium changes) - Reassess anion gap to confirm resolution
Inpatient Diabetes Management
Managing diabetes in hospitalized patients differs significantly from outpatient management. The goal is to prevent hyperglycemia complications while avoiding hypoglycemia.
General Inpatient Principles
Stop Oral Agents
Discontinue all oral diabetes medications upon admission. Their metabolic effects are unpredictable in acute illness. Use insulin-based regimens exclusively.
Key Rules: - Hold all oral antidiabetic agents (metformin, sulfonylureas, GLP-1 agonists, DPP-4 inhibitors) - Type 1 diabetes MUST receive some basal insulin (risk of DKA if omitted) - Type 2 diabetes on insulin alone should resume home dose (adjusted for acute illness) - Type 2 diabetes on oral agents: start sliding scale insulin
Total Daily Insulin (TDI) Calculation
Calculate basal-bolus insulin dosing based on body weight:
$$\text{TDI (units/day)} = 0.4 \text{ units/kg}$$
Alternative for elderly (>70 years), renal insufficiency (Cr >1.5), or tight glycemic control goal: $$\text{TDI} = 0.3 \text{ units/kg}$$
Distribution: - Basal insulin: 50% of TDI given as long-acting insulin (insulin glargine/degludec) once daily at bedtime - Bolus insulin: 50% of TDI divided among meals (roughly 1/3 at each meal)
Example TDI Calculation
Patient: 80 kg male, standard dosing
$$\text{TDI} = 0.4 \times 80 = 32 \text{ units/day}$$
- Basal: Insulin glargine 16 units subcutaneous once nightly
- Bolus: 16 units total distributed at meals
- Breakfast: ~5 units rapid-acting insulin
- Lunch: ~5 units rapid-acting insulin
- Dinner: ~6 units rapid-acting insulin
Supplemental Sliding Scale
Correct for glucose above target with rapid-acting insulin:
$$\text{Supplemental insulin} = \frac{\text{Current BG} - 100}{30} \text{ units}$$
Example: BG 280 mg/dL → (280 - 100)/30 = 6 units additional insulin
Adjusting Insulin Regimen
Review the previous day's blood glucose values and supplemental insulin use:
- Calculate total supplemental insulin given over 24 hours
- Divide by 2: One-half of supplemental insulin increases basal dosing, one-half increases bolus dosing
- Apply adjustment:
- Increase basal insulin by ½ of supplemental amount
- Increase next day's bolus dosing by ½ of supplemental amount
Example: Patient received 20 units total supplemental insulin over 24 hours - Increase basal insulin by 10 units (basal: 16 → 26 units) - Increase bolus insulin by 10 units total (bolus: 16 → 26 units divided among meals)
Glycemic Targets
Prevent Both Extremes
Avoid both hypoglycemia (<70 mg/dL) and excessive hyperglycemia (>300 mg/dL). Tight control (110-140 mg/dL) increases hypoglycemia risk and may increase mortality.
General Hospital Target: 140-180 mg/dL fasting and premeal
ICU Target: 140-180 mg/dL (avoid tight targets <110 mg/dL due to hypoglycemia risk)
Special Populations: - Cardiac ICU: may target slightly tighter (120-160) - Pregnant patients with gestational diabetes: tighter control (fasting <95, 1-hour postmeal <140)
Hyperthyroidism
Hyperthyroidism represents excessive thyroid hormone production. Management depends on etiology and severity.
Etiologic Classification by Radioactive Iodine Uptake
The radioactive iodine uptake (RAIU) scan differentiates hyperthyroid etiologies:
| RAIU Pattern | Likely Diagnosis | Management |
|---|---|---|
| Diffuse uptake | Graves' disease (immune-mediated) | Antithyroid drugs, beta-blockade, or radioactive iodine |
| Heterogeneous uptake | Multinodular goiter (toxic multinodular) | Antithyroid drugs or radioactive iodine |
| Single focus | Toxic nodule (single autonomous nodule) | Radioactive iodine or surgical removal |
| Low/no uptake | Thyroiditis (subacute, viral, post-partum) OR exogenous thyroid hormone | Supportive care; discontinue exogenous hormone if applicable |
Thyroid Storm
Thyroid storm is a rare but life-threatening complication of uncontrolled hyperthyroidism characterized by severe thyrotoxicosis with systemic manifestations.
Medical Emergency
Thyroid storm has mortality approaching 10% even with treatment. Mortality is higher if diagnosis is delayed or treatment is inadequate.
Diagnostic Criteria (not standardized): - High fever (often >39°C) - Extreme tachycardia (often >140 bpm) - Altered mental status (confusion, delirium, coma) - Gastrointestinal symptoms (nausea, vomiting, diarrhea, hepatomegaly) - Precipitants: acute infection, anesthesia, iodine administration, beta-blocker withdrawal
Emergency Management:

Treatment Sequence (CRITICAL - order matters): 1. Beta-blocker first (propranolol) - blocks peripheral conversion T4→T3 AND reduces cardiac manifestations 2. Antithyroid drug (PTU preferred for faster action) - blocks new hormone synthesis 3. Wait 1 hour - allows antithyroid drug to prevent the iodine from being incorporated into new hormone 4. Iodine (Lugol or SSKI) - inhibits release of preformed hormone; NEVER give without antithyroid drug 5. Glucocorticoid (hydrocortisone) - reduces conversion T4→T3 and provides adrenal support 6. Supportive care - cooling measures, aggressive fluid resuscitation, antibiotics if infection present
Hypothyroidism
Hypothyroidism is thyroid hormone deficiency, classified as primary (thyroid gland failure) or secondary (pituitary/hypothalamic failure).
Primary vs Secondary Hypothyroidism
| Parameter | Primary Hypothyroidism | Secondary Hypothyroidism |
|---|---|---|
| Affected level | Thyroid gland | Pituitary or hypothalamus |
| TSH | Elevated | Low or normal |
| Free T4 | Low | Low |
| Common causes | Hashimoto's, iodine deficiency, post-thyroidectomy | Hypopituitarism, pituitary adenoma, post-transsphenoidal surgery |
Etiologies of Primary Hypothyroidism
Most Common: - Hashimoto's thyroiditis - autoimmune thyroid destruction, anti-TPO/anti-thyroglobulin antibodies - Iodine deficiency - world's most common preventable cause - Post-ablative - radioactive iodine, surgery, external radiation
Medication-Induced: - Antithyroid drugs (propylthiouracil, methimazole) - Amiodarone (high iodine content) - Lithium - Thionamides - Beta-interferon, interleukin-2
Clinical Stages
Early/Subclinical Hypothyroidism: - Elevated TSH with normal free T4 - Often asymptomatic - Screen for cardiac risk factors before treating
Overt Hypothyroidism: - Elevated TSH with low free T4 - Fatigue and lethargy - Cold intolerance - Weight gain (average 5-10 pounds) - Constipation, dry skin, hair loss - Bradycardia, decreased cardiac contractility
Myxedema (Severe Hypothyroidism): - Severe metabolic slowing - Facial and periorbital edema - Pleural effusions, ascites, pericardial effusion - Altered mental status - Severe bradycardia and hypotension
Myxedema Coma (Rare, Medical Emergency): - Life-threatening complication of profound, untreated hypothyroidism - Extreme bradycardia, hypotension, hypothermia - Altered consciousness progressing to coma - Often triggered by infection, anesthesia, or medication
Hypothyroidism Treatment
| Clinical Scenario | Levothyroxine Dosing | Recheck TSH | Special Considerations |
|---|---|---|---|
| New diagnosis, uncomplicated | 1.7 mcg/kg/day (~100-125 mcg for average adult) | 6-8 weeks | Adjust by 25-50 mcg increments based on TSH |
| Elderly or cardiac risk | Start lower: 0.3-0.5 mcg/kg/day (~25-50 mcg) | 6-8 weeks | Titrate slowly to avoid cardiac stress |
| Severe hypothyroidism with cardiac disease | Start very low: 12.5-25 mcg daily | 4-6 weeks | May need stress testing before treatment |
| Myxedema coma | ICU care: loading dose 200-400 mcg IV then 50-100 mcg IV daily | Continuous monitoring | Add T3 (liothyronine 5-20 mcg q4-6h IV) if unstable |
Myxedema Coma Management
Medical Emergency
Myxedema coma requires ICU admission and intensive monitoring. Mortality exceeds 50% even with treatment.
Immediate Interventions:
- IV Levothyroxine Loading: 200-400 mcg IV bolus, then 50-100 mcg IV once daily
- Bypass GI absorption; IV route preferred for reliable delivery
-
Loading dose rapidly repletes central hormone stores
-
Add Liothyronine (T3) if Unstable:
- 5-20 mcg IV q4-6h
- T3 has more rapid action than T4
-
Use in severely ill/cardiovascular unstable patients
-
Empiric Hydrocortisone:
- 100 mg IV q6-8h initially
- Prevents adrenal crisis (adrenal insufficiency may coexist)
-
Taper as clinical improvement occurs
-
Supportive Care:
- Passive external rewarming (avoid active rewarming - can cause shock)
- Mechanical ventilation if respiratory depression
- Careful fluid administration (avoid fluid overload; myxedema patients have total body water excess)
-
Treat precipitant (infection with antibiotics, manage medication withdrawal, etc.)
-
Monitoring:
- Continuous cardiac monitoring (risk of arrhythmias)
- Frequent vital signs
- Serial TSH and free T4 levels
- Transition to oral levothyroxine when stable and able to tolerate PO
Adrenal Insufficiency
Adrenal insufficiency results from inadequate cortisol and/or aldosterone production. Recognition is essential to prevent life-threatening hypotension and electrolyte abnormalities.
Classification
Primary Adrenal Insufficiency (Addison's Disease): - Direct adrenal gland failure - Low cortisol, elevated ACTH (appropriate response) - Loss of both cortisol and aldosterone
Secondary Adrenal Insufficiency: - Pituitary or hypothalamic failure - Low cortisol, low ACTH (inappropriately low response) - Aldosterone production preserved
Common Etiologies
Primary Adrenal Insufficiency: - Autoimmune - 70% of cases in developed countries - Tuberculosis - most common cause worldwide - Vascular - hemorrhage (sepsis, anticoagulation), thrombosis - Metastatic disease - lung, breast, lymphoma - Medications - azole antifungals, etomidate (single doses can cause adrenal suppression)
Secondary Adrenal Insufficiency: - Chronic glucocorticoid use - most common cause - Pituitary adenoma or apoplexy - Hypothalamic/pituitary surgery or radiation - Traumatic brain injury
Clinical Presentation
Acute Adrenal Crisis: - Profound hypotension (often <80 mmHg systolic) - Tachycardia with severe symptoms - Severe dehydration - Hyponatremia and hyperkalemia - Abdominal pain with or without acute abdomen finding - Altered mental status - Fever (infection may be precipitant)
Chronic Primary Adrenal Insufficiency: - Fatigue and weakness - Hyperpigmentation (from elevated ACTH) - Salt craving - Weight loss - Orthostatic hypotension
Chronic Secondary Adrenal Insufficiency: - Fatigue and weakness - Hypoglycemia (loss of cortisol's counter-regulatory effect) - No hyperpigmentation (ACTH not elevated) - Often subtle presentation
Diagnostic Approach
Screening - Early Morning Cortisol: - Cortisol <5 μg/dL - highly suggestive of insufficiency (further testing needed) - Cortisol >18 μg/dL - adequately rules out insufficiency - Cortisol 5-18 μg/dL - borderline, requires confirmatory testing
Confirmation - ACTH Stimulation Test (Cosyntropin Test): - Administer cosyntropin 250 mcg IV - Measure cortisol at baseline, 30, and 60 minutes - Normal response: cortisol rises to >20 μg/dL - Abnormal: cortisol <18-20 μg/dL at 30-60 minutes = AI confirmed
Differentiate Primary vs Secondary: - Elevated ACTH (>100 pg/mL) = Primary insufficiency - Low or normal ACTH = Secondary insufficiency
Localize Secondary Insufficiency: - Primary insufficiency: abdominal CT (assess for TB, hemorrhage, adrenal enlargement) - Secondary insufficiency: brain MRI (assess pituitary, hypothalamic structure)
Acute Adrenal Crisis Management
Life-Threatening Emergency
Do not wait for confirmatory testing in suspected acute adrenal crisis. Start glucocorticoids immediately - risk of not treating far outweighs risk of inappropriate treatment.

Immediate Interventions:
- Hydrocortisone IV:
- Initial: 100 mg IV bolus immediately
- Maintenance: 50-100 mg IV q6h × first 24 hours
-
Taper over 1-3 days as clinical stability improves
-
Aggressive Fluid Resuscitation:
- Normal saline 1-2 L in first 1-2 hours
- Additional 1-2 L over 2-4 hours
- Restore intravascular volume, correct hyponatremia through dilution
-
Avoid hypotonic fluids (worsens hyponatremia)
-
Identify and Treat Precipitant:
- Sepsis: broad-spectrum antibiotics after cultures
- Medication withdrawal: resume medication
-
Surgery/trauma: continue hydrocortisone coverage
-
Monitoring and Transition:
- Continuous cardiac monitoring (hypokalemia risk)
- Monitor BP, heart rate, electrolytes
- As hemodynamically stable, begin oral glucocorticoid replacement
- Usually transition to prednisone 5-10 mg daily
Chronic Adrenal Insufficiency Maintenance
Glucocorticoid Replacement: - Prednisone 5 mg each morning (matches normal cortisol production) - Or hydrocortisone 15-25 mg divided (15 mg AM, 5-10 mg PM) - Adjust based on clinical response
Mineralocorticoid Replacement (Primary AI only): - Fludrocortisone 0.05-0.2 mg once daily - Goal: maintain BP, normalize sodium and potassium - Essential in primary insufficiency; NOT needed in secondary
Sick Day Rules: - During acute illness, fever, surgery: increase glucocorticoid dose 2-3 fold - Infection: 50-100 mg hydrocortisone q6-8h or prednisone 20-30 mg q6-8h - Resume baseline dosing when acute illness resolves
Emergency Preparedness: - Provide patient with dexamethasone 4 mg IM prefilled syringe for emergency use - Medic-Alert bracelet/card - Written emergency action plan - Educate family members on recognition and emergency management
Key Management Points
Prevention of Crisis
Patient education about stress-dosing, recognizing symptoms, and emergency access to medications prevents most adrenal crises. Patients must understand they require lifelong replacement therapy and cannot stop medications suddenly.
Patient Education: - Adrenal insufficiency is a chronic condition requiring lifelong treatment - NEVER discontinue glucocorticoids without medical supervision - Increase dose during stress, illness, or fever - Always carry emergency glucocorticoid (dexamethasone syringe) - Wear medical alert identification - Notify all healthcare providers of condition before any procedures
Neurology: Essential Evaluation Frameworks
Evaluation of Headache
History and Presenting Features
A systematic headache history requires understanding the temporal pattern and character of pain. Begin by establishing onset timing—whether symptoms developed suddenly over seconds to minutes or gradually over hours to days. This temporal relationship often guides your diagnostic thinking. Characterize the pain quality using patient language: pressure, throbbing, stabbing, or burning sensations provide clues. Determine location with precision, noting whether pain is unilateral or bilateral, frontal, temporal, occipital, or generalized.
Establish severity using a numeric scale (0-10), duration of individual episodes and total illness duration, and identifiable triggers such as stress, sleep deprivation, menses, or positional changes. Explore associated symptoms systematically: floaters or visual changes, nausea and vomiting, photophobia and phonophobia, and any focal neurologic deficits.
Red Flag Symptoms Requiring Urgent Evaluation
Headache Red Flags
- Focal neurologic deficit or weakness
- Altered mental status or confusion
- Seizure activity
- Vision changes or diplopia
- Meningeal signs (neck stiffness)
- Fever
- Positional relationship to symptoms
- Progressive worsening
- Papilledema on fundoscopy
- Thunderclap onset (sudden maximal intensity)
Primary Headache Disorders
| Headache Type | Characteristics | Typical Triggers | Treatment |
|---|---|---|---|
| Tension | Bilateral pressure or band-like sensation; mild to moderate severity; no prodrome | Stress, sleep deprivation, muscle tension | NSAIDs, acetaminophen; tricyclic antidepressants (amitriptyline) for chronic |
| Cluster | Unilateral periorbital/temporal pain; autonomic features (rhinorrhea, conjunctival injection, lacrimation, miosis, ptosis) | Alcohol, nitrates | High-flow oxygen (15L/min); subcutaneous sumatriptan; prednisone 60mg once daily for acute cluster |
| Migraine | Unilateral throbbing pain; often preceded by aura (visual, sensory, speech); 4-72 hour duration; nausea/vomiting | Hormonal changes, sleep disruption, weather changes | Triptans (5HT1 agonists); acetaminophen + caffeine combinations; IV options (DHE, ketorolac) for severe episodes |
Secondary Headache Causes
| Category | Conditions | Key Distinguishing Features |
|---|---|---|
| Traumatic | Post-concussive headache, subarachnoid hemorrhage, subdural hematoma | Recent head trauma; thunderclap onset for SAH |
| Increased ICP | Brain tumor, hydrocephalus, pseudotumor cerebri | Progressive symptoms, morning symptoms, papilledema |
| Decreased ICP | Post-lumbar puncture, CSF leak | Recent LP or dural puncture; positional quality |
| Vascular | Acute stroke, arterial dissection, vasculitis, temporal arteritis | Age >50, focal deficits, vision loss, jaw claudication |
| Meningeal | Bacterial meningitis, viral meningitis, subarachnoid hemorrhage | Fever, neck stiffness, photophobia |
| Extracranial | Sinusitis, temporomandibular joint dysfunction, glaucoma | Facial pressure, jaw pain, eye pain with vision changes |
| Systemic | Hypoxia, uncontrolled hypertension, hypoglycemia | Associated systemic symptoms |
| Medication-Related | Medication overuse headache, withdrawal syndromes | Frequent analgesic use; recent medication changes |
Diagnostic Approach
Headache Workup Strategy
- Imaging First: Non-contrast CT brain for acute presentation with concerning features (thunderclap, focal deficits, altered mental status)
- MRI Brain: When structural lesion suspected but CT normal; migraines with atypical features
- Lumbar Puncture: If febrile with meningeal signs or suspected SAH with negative CT imaging
- Labs: ESR and CRP for temporal arteritis suspicion (especially age >50)
- Specialty Imaging: CTA/MRA for vascular concerns; CT sinuses for sinusitis
Evaluation of Syncope
Syncope results from transient cerebral hypoperfusion. Understanding the mechanism guides management and risk stratification. The WOMAN PE framework organizes the major etiologic categories.
Syncope Etiology Framework: WOMAN PE
| Category | Mechanism | Clinical Features |
|---|---|---|
| W - Neurally Mediated | Vagal/neural reflex activation | Prodromal symptoms (palpitations, nausea, diaphoresis); recurrent episodes; situational or positional triggers |
| O - Orthostatic | Inability to maintain blood pressure on position change | Symptoms with standing; improvement with lying down; often elderly or dehydrated |
| M - Mechanical (FATAL) | Structural obstruction to cardiac output | Exertional onset; cardiac murmur; no prodrome; family history of sudden death |
| A - Arrhythmia (FATAL) | Abnormal heart rhythm | Sudden onset without prodrome; palpitations; syncope during sleep possible |
| V - Vascular | Acute vascular compromise | Focal neurologic deficits; chest pain; risk factors for dissection |
| P - Psychiatric | Psychogenic non-epileptic seizure (pseudoseizure) | Gradual onset; variable presentation; often younger patients |
| E - Endocrine/Other | Metabolic or medication-related | Hypoglycemia, electrolyte abnormalities, medication effects |
Evaluation by Etiology
| Etiology | Initial Testing | Additional Workup |
|---|---|---|
| Neurally Mediated | Orthostatic vital signs; history of prodrome | Tilt table test if diagnosis uncertain; conservative management |
| Orthostatic | Supine/standing blood pressure (≥20 mmHg systolic or ≥10 mmHg diastolic drop); assess volume status | IV fluid repletion; compression stockings; medication review |
| Mechanical (Exertional, Murmur) | ECG; cardiac auscultation | Transthoracic echocardiography; cardiology consultation |
| Arrhythmia | 12-lead ECG; continuous telemetry | Holter monitor; event monitor; electrophysiology consultation |
| Vascular (Focal Deficits) | Careful neurologic examination | CTA neck/chest; carotid ultrasound; neurology consultation |
Comprehensive Syncope Workup
Syncope Investigation Protocol
- Labs: CBC, comprehensive metabolic panel, glucose level, pregnancy test (if applicable)
- Cardiac: 12-lead ECG, continuous telemetry monitoring, troponin
- Imaging: Chest X-ray; consider D-dimer if VTE suspected; consider troponin elevation
- Specialized: EEG if seizure suspected; carotid ultrasonography; brain imaging if focal deficits
- Risk Stratification: Presence of cardiac etiology indicates higher risk of adverse outcomes
Altered Mental Status and Delirium
Delirium represents acute dysfunction of consciousness and cognition. Understanding the spectrum of mental status changes and systematic etiologic search are essential.
Spectrum of Altered Mental Status
Progress from hyperalert (agitation, hallucinations) through confusion and true delirium, then to progressive somnolence: lethargic (falls asleep easily but awakens to stimulation), obtunded (awakens only to vigorous stimulation), stuporous (minimal response to painful stimuli only), and finally comatose (no purposeful response to external stimuli).
Etiologic Framework: "HE STOPS for TIPS on AEIOUS"
- H: Hepatic encephalopathy, Hypertensive emergency
- E: Electrolyte abnormalities
- S: Stroke, Subdural hematoma, Subarachnoid hemorrhage
- T: Trauma, Temperature extremes
- O: Opioid toxicity, Overdose of other medications
- P: Psychiatric illness
- S: Seizure activity, Sepsis, Syphilis (neurosyphilis)
- T: Thyroid dysfunction (hyper and hypothyroid), Toxic ingestion
- I: Infection (UTI, pneumonia, meningitis), Intracranial process, Increased ICP
- P: Porphyria
- S: Systemic acidosis
- A: Anemia, Anoxia, Acidosis
- E: Endocrine disorders (hypoglycemia, DKA, HHS)
- I: Intoxication (alcohol, drugs), Intracranial hemorrhage
- O: Opioid toxicity, Oxygen hypoxia, Osmolality (hyponatremia)
- U: Uremia
- S: Seizure, Stroke, Subdural
Glasgow Coma Scale
The GCS quantifies level of consciousness using eye opening, verbal response, and motor response.
| Component | Scoring (out of 15 total) |
|---|---|
| Eye Opening (E: 1-4) | 4 = Spontaneous; 3 = To verbal command; 2 = To pain; 1 = No response |
| Verbal Response (V: 1-5) | 5 = Oriented; 4 = Confused; 3 = Inappropriate words; 2 = Incomprehensible; 1 = No response |
| Motor Response (M: 1-6) | 6 = Obeys commands; 5 = Localizes to pain; 4 = Withdraws from pain; 3 = Abnormal flexion; 2 = Abnormal extension; 1 = No response |
Interpretation: 15 = Normal function; 13-14 = Minor impairment; 9-12 = Moderate impairment; ≤8 = Severe impairment/comatose state
Neurologic Examination in Altered Mental Status
| Exam Component | Findings and Interpretation |
|---|---|
| Mental Status | Document GCS score; assess orientation to person, place, time; evaluate attention and memory |
| Pupils | Pinpoint = opioid intoxication or pontine hemorrhage; mid-fixed = midbrain injury; dilated and fixed = anoxic injury, herniation, or anticholinergic toxicity |
| Extraocular Movements | Doll's eyes (oculocephalic reflex) and cold calorics (oculovestibular reflex) assess brainstem function; absence suggests brainstem injury |
| Motor/Sensory | Assess for focal deficits suggesting stroke; check for meningeal signs (neck stiffness, Kernig, Brudzinski) |
| Reflexes | Brisk reflexes may suggest metabolic derangement; diminished reflexes suggest toxic ingestion |
Diagnostic Workup
AMS Investigation Sequence
- Universal Labs: CBC, comprehensive metabolic panel, urinalysis (all patients)
- Toxins: Urine drug screen, blood alcohol level
- Targeted Labs (based on history/exam):
- Hepatic encephalopathy: serum ammonia, liver function tests
- Endocrine: TSH, serum/urine osmolality, cortisol
- Nutritional: B12 level, folate
- Acidosis: arterial blood gas
- Imaging: Non-contrast CT head for acute presentation; MRI if CT normal but high suspicion for structural disease
- Lumbar Puncture: If meningitis/encephalitis suspected after imaging excludes mass
- EEG: For suspected seizure activity; encephalitis; myxedema coma
Management Principles
Acute AMS Management
- Discontinue any medication that could precipitate altered mental status
- Administer thiamine 100 mg IV (prevents Wernicke encephalopathy)
- Administer dextrose (D50) if hypoglycemia present (after thiamine to prevent Wernicke)
- Consider naloxone if opioid intoxication suspected
- Maintain cervical spine immobilization if trauma concern
- Elevate head of bed and manage increased ICP if indicated
Evaluation of Stroke
Stroke represents acute neurologic deficit from vascular origin. Rapid identification of stroke type and vascular territory guides acute intervention.
Stroke Classification
- TIA (Transient Ischemic Attack): Transient neurologic symptoms with negative imaging; resolution within 24 hours
- Ischemic Stroke (85% of cases):
- Embolic: Cardioembolic source (atrial fibrillation, valvular disease); arterial embolus
- Thrombotic: Atherosclerotic disease; lacunar infarction
- Hemorrhagic Stroke (15% of cases):
- Intracerebral hemorrhage (hypertension, amyloid angiopathy)
- Subarachnoid hemorrhage (ruptured aneurysm, AVM)
Vascular Territory and Clinical Syndromes
| Vessel | Territory | Clinical Presentation |
|---|---|---|
| ICA/Ophthalmic | Retina | Amaurosis fugax (transient monocular vision loss) |
| ACA (Anterior Cerebral Artery) | Medial frontal/parietal | Leg hemiplegia > arm; urinary incontinence; personality change |
| MCA (Middle Cerebral Artery) | Lateral cortex/basal ganglia | Face/arm hemiplegia > leg; aphasia (dominant hemisphere) or neglect (nondominant) |
| PCA (Posterior Cerebral Artery) | Occipital lobe | Homonymous hemianopia with macular sparing; visual hallucinations |
| Vertebral/PICA (Wallenberg) | Lateral medulla | Ipsilateral facial numbness; contralateral body numbness; Horner syndrome; intractable hiccups |
| Basilar Artery | Brainstem (pons, midbrain) | Locked-in syndrome (at midbrain level); quadriplegia; CN abnormalities; altered consciousness |
| Cerebellar | Cerebellum | Vertigo, nausea/vomiting; diplopia; ipsilateral ataxia; headache |
| Lacunar | Small penetrating vessels | 5 classic syndromes: pure motor; pure sensory; ataxic hemiparesis; dysarthria-clumsy hand; mixed sensorimotor |
NIH Stroke Scale (NIHSS)
The NIHSS quantifies stroke severity across 11 items (1a through 11). Reference the NIH Stroke Scale on MDCalc for detailed scoring. Higher scores correlate with larger infarct volume and worse outcomes.
Acute Stroke Diagnostic Workup
Stroke Evaluation Protocol
- Labs: CBC, comprehensive metabolic panel, coagulation studies (PT/PTT), ECG, troponin, toxicology screen
- Monitoring: Continuous cardiac telemetry
- Imaging: Stat non-contrast CT head (rule out hemorrhage); CTA head/neck if large vessel occlusion symptoms present
- ICU Criteria: tPA recipients; worsening strokes; hemorrhagic strokes; requiring vasopressor support
tPA Eligibility Criteria
Alteplase (tPA) represents standard care for eligible acute ischemic stroke.
tPA Contraindications and Timing
- Timing: Within 4.5 hours from symptom onset
- Blood Pressure: Must be <185/110 mmHg (uncontrolled hypertension is absolute contraindication)
- Platelet Count: ≥100,000 (severe thrombocytopenia contraindication)
- Coagulation: INR ≤1.7 if on warfarin
- Bleeding Risk: No recent surgery, intracranial hemorrhage, GI bleeding, or active bleeding
- Other: No seizure at stroke onset; blood glucose >50 and <400 mg/dL
Musculoskeletal: Evaluation and Management
Evaluation of Back Pain
Back pain affects the majority of adults during their lifetime. Systematic evaluation distinguishes mechanical causes from serious underlying pathology.
Red Flag Assessment
Back Pain Red Flags Requiring Urgent Evaluation
- Recent significant trauma (fall from height, motor vehicle accident)
- Age greater than 50 years with new-onset back pain
- History of cancer or current malignancy
- Unexplained weight loss
- Fever suggesting infection
- Progressive neurologic deficits
- Bowel or bladder dysfunction (suggests cauda equina)
- IV drug use (increased infection risk)
- Immunosuppression or chronic corticosteroid use
- Severe osteoporosis or prolonged corticosteroid therapy
Categorization of Back Pain Etiology
Mechanical Back Pain (Most Common ~80%)
Mechanical etiologies account for the vast majority of back pain presentations. Muscle strain develops acutely, often after lifting or unusual activity, with localized muscular tenderness and no radiation. Degenerative disc disease and facet arthropathy produce chronic pain, often with positional components (worse with extension for facet disease). Lumbar strain typically responds to rest, NSAIDs, and physical therapy.
Non-Mechanical Back Pain (~10-20%)
Serious etiologies require imaging and urgent intervention. Malignancy in the vertebral column or epidural space presents with progressive pain, weight loss, and constitutional symptoms. Infection (epidural abscess, vertebral osteomyelitis) typically accompanies fever and systemic illness, particularly in immunocompromised hosts. Inflammatory conditions (ankylosing spondylitis, reactive arthritis) feature inflammatory markers and systemic symptoms. Referred pain from abdominal organs (ruptured AAA, renal pathology, pancreatitis) must not be overlooked.
Cauda Equina Syndrome: The Surgical Emergency
Cauda equina syndrome represents compression of multiple lumbosacral nerve roots in the spinal canal. This surgical emergency requires recognition and urgent decompression to prevent permanent neurologic injury.
Cauda Equina Syndrome: Classic Presentation
- Saddle Anesthesia: Loss of sensation in buttocks, perineum, and inner thighs (S3-S5 dermatomes)
- Bilateral Lower Extremity Weakness or Radiculopathy
- Urinary Retention or urinary incontinence with overflow
- Bowel Dysfunction: Loss of sphincter control
- Severe Lower Back Pain with bilateral leg pain
Immediate Action: Stat MRI lumbar spine; emergency neurosurgical consultation; surgical decompression within hours of symptom onset
Diagnostic Approach to Back Pain
Back Pain Evaluation Strategy
- No Red Flags: Conservative management with NSAIDs, physical therapy, activity modification; reassess in 4-6 weeks
- Red Flags Present: Imaging workup indicated
- X-ray: Initial imaging for fracture, alignment, degenerative changes
- MRI: Gold standard for soft tissue, nerve compression, myelopathy; assess for cauda equina
- Labs if infection/malignancy suspected: ESR, CRP, CBC, blood cultures
- Red Flag Combinations:
- Fever + IV drug use → MRI + blood cultures for vertebral osteomyelitis/abscess
- Cancer history + weight loss → MRI for metastatic disease
- Progressive neurologic deficit → Urgent MRI for myelopathy or cauda equina
Evaluation of Joint Pain
Joint pain represents inflammation, mechanical dysfunction, or systemic disease. Characterization as monoarticular, oligoarticular (2-4 joints), or polyarticular (≥5 joints) guides differential diagnosis.
Inflammatory vs Mechanical Joint Pain
Key distinguishing feature: Morning stiffness lasting ≥30 minutes suggests inflammatory arthritis.
- Inflammatory: Symmetric polyarticular pattern; morning stiffness; systemic symptoms (fever, malaise); elevated inflammatory markers
- Mechanical: Monoarticular or asymmetric; activity-related worsening; no systemic symptoms; normal inflammatory markers
Monoarticular Arthritis Differential
| Condition | Typical Joint | Presentation | Key Finding |
|---|---|---|---|
| Gout | First MTP (hallux), ankle, knee | Acute severe pain; red, warm, swollen | Negatively birefringent monosodium urate crystals; male predominance; diuretic use |
| Pseudogout (CPPD) | Knee (most common) | Similar to gout but generally milder | Positively birefringent calcium pyrophosphate crystals; older patients |
| Septic Arthritis | Knee (most common); hip in young children | Acute monoarticular pain; fever; refusal to bear weight | Medical emergency; requires arthrocentesis and empiric antibiotics |
| Traumatic | Variable | Recent injury; mechanical symptoms | History of trauma; imaging findings |
Polyarticular Arthritis Differential
| Condition | Joint Pattern | Additional Features | Lab Findings |
|---|---|---|---|
| Rheumatoid Arthritis | Symmetric PIP, MCP, wrists | Morning stiffness >1 hour; hand deformities with chronicity | RF+ or anti-CCP+; elevated ESR/CRP |
| Systemic Lupus Erythematosus | Hands, wrists, knees | Malar rash, photosensitivity, oral ulcers, Raynaud | ANA+; low complement; thrombocytopenia |
| Viral Arthritis | Symmetric hands, wrists | Recent viral illness; self-limited | Viral serology; normal inflammatory markers initially |
| Reactive Arthritis | Lower extremities | Recent GI or GU infection; asymmetric | HLA-B27+; elevated inflammatory markers |
Synovial Fluid Analysis
Arthrocentesis with synovial fluid analysis distinguishes inflammatory from non-inflammatory arthritis and identifies crystal arthropathy or infection.
| Fluid Type | Appearance | WBC Count | PMN % | Interpretation |
|---|---|---|---|---|
| Normal | Clear | <200 | <25% | Normal joint fluid |
| Non-inflammatory | Clear to slightly turbid | 200-2000 | <25% | OA, mechanical dysfunction |
| Inflammatory | Cloudy | 2000-50000 | >50% | RA, SLE, crystalline arthritis, viral |
| Septic | Purulent/turbid | >50000 (often >100000) | >75% | Medical emergency; culture essential |
Crystal Analysis
- Gout: Monosodium urate crystals; needle-shaped; negatively birefringent (appear yellow under parallel light)
- Pseudogout (CPPD): Calcium pyrophosphate dihydrate crystals; rhomboid/rod-shaped; positively birefringent (appear blue under parallel light)
Septic Arthritis: Critical Management
Septic arthritis represents a medical emergency. Staphylococcus aureus causes approximately 50% of non-gonococcal septic arthritis. Neisseria gonorrhoeae predominates in sexually active young adults. Rapid diagnosis and treatment prevent permanent joint damage.
Septic Arthritis Management Protocol
- Diagnosis: Immediate arthrocentesis with synovial fluid studies (cell count, differential, Gram stain, culture, crystals, glucose)
- Empiric Antibiotics (start immediately, don't wait for culture):
- Vancomycin 15-20 mg/kg IV q8-12h + Ceftriaxone 2g IV q12h
- Adjust based on Gram stain and culture results (typically 2-4 weeks of IV antibiotics)
- Source Control: Repeated arthrocentesis or arthroscopic drainage for large effusions or if clinical deterioration
- Imaging: X-ray to exclude fracture; consider ultrasound for hip arthrocentesis
Approach to Polyarticular Arthritis
When evaluating polyarticular joint pain, consider the pattern (symmetric vs asymmetric), duration (acute vs insidious), and presence of systemic features.
Diagnostic Algorithm
Polyarticular Arthritis Workup
- Clinical Assessment:
- Timeline of onset (acute <6 weeks; insidious >6 weeks)
- Joint distribution pattern
- Morning stiffness duration
- Systemic symptoms
- Labs:
- Inflammatory markers (ESR, CRP)
- Rheumatologic panel (RF, anti-CCP, ANA, complement levels)
- Infectious workup if indicated (viral serology, cultures)
- Imaging:
- X-rays of affected joints (assess for erosions suggesting RA)
- Ultrasound for effusion documentation
- Arthrocentesis: If diagnostic uncertainty or monoarticular component with fever
Special Populations
Young Woman with Polyarthritis: Consider SLE in differential. Screen with ANA, CBC (thrombocytopenia, leukopenia), and urinalysis (proteinuria/hematuria).
Older Adult with Acute Polyarthritis: Consider viral arthritis (parvovirus, hepatitis C), crystal arthropathy, and polymyalgia rheumatica (ESR >50, temporal headache).
IV Drug User with Monoarthritis: Rule out septic arthritis with empiric antibiotics while awaiting culture; screen for endocarditis.
Outpatient Pearls: Prevention, Screening, and Immunization
Preventive medicine represents the cornerstone of outpatient internal medicine practice. Evidence-based screening and immunization prevent disease progression and reduce morbidity and mortality.
Disease Screening Guidelines
The United States Preventive Services Task Force (USPSTF) provides evidence-based recommendations for population-level screening. Implementing these recommendations improves outcomes while minimizing unnecessary testing.
Cancer Screening
| Cancer Type | Screening Test | Age to Begin | Age to Stop | Screening Interval | Notes |
|---|---|---|---|---|---|
| Colorectal | Colonoscopy or other modalities (FIT, sigmoidoscopy, CT colonography) | 45 | 75 | Every 10 years for colonoscopy | USPSTF lowered starting age from 50 to 45 in 2021; shared decision for 76-85 |
| Breast | Mammography | 50 (shared decision 40-49) | 74 | Every 2 years | Risk stratification affects frequency; discuss benefits/harms |
| Cervical | Pap smear alone or Pap+HPV | 21 (start age) | 65 (stop age) | Every 3 years (Pap); Every 5 years (Pap+HPV) | HPV vaccination reduces screening need; hysterectomy without CIN stops screening |
| Lung | Low-dose CT (LDCT) | 50 | 80 | Annual screening | Requires ≥20 pack-year history; benefit for former smokers within 15 years of quitting |
| Prostate | PSA testing | 55 (shared decision 40-69) | 70 | Depends on baseline | High variability in recommendations; discuss individual risk/preference |
Metabolic and Cardiovascular Screening
| Condition | Screening Test | Population | Frequency | Key Considerations |
|---|---|---|---|---|
| Type 2 Diabetes | Fasting glucose or HbA1c | Age 35-70; BMI ≥25 or overweight | Every 3 years if normal | Screen younger if additional risk factors (family history, prior GDM) |
| Hypertension | Blood pressure measurement | Age 18+ | Annually or at each visit | Home BP monitoring recommended; confirm elevated readings |
| Lipids | Fasting lipid panel | Age 20+ | 4-6 years (varies by risk) | More frequent if known cardiovascular disease or lipid abnormality |
| Abdominal Aortic Aneurysm (AAA) | Abdominal ultrasound, one-time | Men age 65-75 who ever smoked | One-time screening only | Not recommended for never-smokers; not recommended in women |
| Atherosclerotic CVD | Assess 10-year risk using calculator | Age 40-75 | Periodically | Framingham or pooled cohort equations inform statin initiation |
Infectious Disease Screening
| Infection | Screening Test | Population | Frequency | Management if Positive |
|---|---|---|---|---|
| Hepatitis C Antibody | Anti-HCV antibody, confirmatory HCV RNA | All adults age 18-79 | One-time minimum | Refer for treatment if RNA positive; all HCV curable with DAA therapy |
| HIV | 4th generation antigen/antibody test | All age 15-65; higher risk more frequently | At least once in lifetime; annual for higher-risk populations | Urgent antiretroviral therapy; long-term suppression possible |
| Syphilis | RPR/VDRL with FTA-ABS or TP-PA confirmatory | High-risk populations; all pregnant women | Based on risk; annual for MSM | Early treatment prevents progression; latent syphilis still infectious |
| Tuberculosis | TST (tuberculin skin test) or IGRA (interferon-gamma release assay) | Contacts of TB cases; recent immigrants from endemic areas | As indicated | Treat latent TB to prevent active disease |
Osteoporosis and Bone Health
| Screening | Population | Method | Frequency | Treatment Threshold |
|---|---|---|---|---|
| Osteoporosis | Women ≥65; men ≥70; postmenopausal women <65 with risk factors | DEXA scan (dual-energy X-ray absorptiometry) | Every 2 years if T-score -1.0 to -2.5; annual if T-score <-2.5 | T-score ≤-2.5 or T-score -1 to -2.5 with risk factors |
Mental Health and Substance Abuse Screening
| Condition | Screening Tool | Population | Positive Result Management |
|---|---|---|---|
| Depression | PHQ-9 (Patient Health Questionnaire-9) or shorter PHQ-2 | All adults; more frequent in chronic disease | Refer for counseling; consider antidepressant therapy |
| Alcohol Misuse | AUDIT (Alcohol Use Disorders Identification Test) or AUDIT-C (3-item version) | All adults | Counsel on reduction; refer to addiction specialist if SUD diagnosed |
| Drug Use | NIDA Quick Screen or OARRS (prescription drug monitoring program) | All adults; mandatory in opioid-prescribing practices | Urine drug screening; refer to addiction services; avoid opioid prescribing |
| Intimate Partner Violence | HARK or other validated screening | All women; men if available resources | Safety assessment; referral to social work and community resources |
Immunization Schedules and Recommendations
Vaccination represents one of medicine's greatest public health achievements. Adult immunization schedules change regularly based on emerging evidence and epidemiology.
Core Adult Immunizations
| Vaccine | Schedule | Target Population | Booster/Revaccination | Special Populations |
|---|---|---|---|---|
| Influenza (Flu) | Annual single dose (most adults) | All adults ≥6 months; especially ≥65 or chronic disease | Annual fall/early winter | High-dose or adjuvanted for ≥65 |
| Tdap | One-time dose if not previously given | All adults, especially if >10 years since last Td | Td booster q10 years | Pregnant women get Tdap; non-pregnant can get Td |
| Pneumococcal - PCV20 | Single dose given to all ≥65 or high-risk | All ≥65; chronic lung/heart disease; diabetes; smoking; CSF leak | No revaccination if PCV20 given | Can follow with PPSV23 per guidelines if prior PPSV23 given |
| Pneumococcal - PCV15+PPSV23 | PCV15 now, PPSV23 in 1 year (if not prior) | Age 65+; chronic disease; smoking | ≥1 year between PCV15 and PPSV23 | Algorithm more complex for prior PPSV23 recipients |
| Shingles (Shingrix) | Two doses, 2-6 months apart | All ≥50; immunocompetent individuals | No booster needed | Prior Zostavax recipients should get Shingrix |
| Hepatitis B | 3-dose series (standard) or 2-dose (high-dose Heplisav-B) | All non-immunized adults; age 19-59 routinely; ≥60 at risk or shared decision | Consider anti-HBs testing to confirm response | Immunocompromised may need higher doses or additional doses |
| HPV (Gardasil-9) | 2 or 3-dose series depending on age | Through age 26 (routinely); shared decision-making ages 27-45 | None standard; may revaccinate in special situations | Dosing: 2 doses if started at age 12-14; 3 doses if started ≥15 or immunocompromised |
| COVID-19 | Primary series then boosters | All age 6 months+ | Boosters per current epidemiology; frequency variable | Immunocompromised require additional primary doses + boosters |
| Varicella | 2 doses, 4+ weeks apart | Non-immune adults; no prior vaccination or serology negative | No routine booster | Contraindicated in pregnancy; wait 4 weeks before pregnancy |
| Measles, Mumps, Rubella (MMR) | 1-2 doses depending on birth year; non-immune adults | All without immunity; born 1957+ benefit from 2 doses | No routine booster | Contraindicated in pregnancy; check immunity status first |
High-Risk Population Immunizations
| Vaccine | Indication | Schedule | Special Considerations |
|---|---|---|---|
| Hepatitis A | Chronic liver disease, HAV non-immune, MSM, IVDU, travel | 2 doses, 6-12 months apart | Some combination vaccines available (Hep A + B) |
| Meningococcal (MenACWY) | Age 16-23 (1 or 2 doses depending on product); college students; asplenic; terminal complement deficiency | Based on vaccine type and risk | Serogroup B requires separate vaccine |
| Meningococcal B (Bexsero/Menhibrix) | Asplenic patients, complement deficiency, MenB outbreaks | 2 doses, 1 month apart | Separate from MenACWY; time intervals matter |
| Pneumococcal (PPSV23) | Chronic disease, smoking, age 65+, asplenic, immunocompromised | 1 dose; may repeat ≥1 year later if immunocompromised | Now often follows PCV20 or PCV15 |
| Tuberculosis (BCG) | Only in non-immunized healthcare workers with frequent TB exposure | Single dose | Not routinely given in US; rare use |
| Yellow Fever | Travel to endemic areas; occupational exposure | Single dose; booster q10 years for ongoing risk | Consult travel medicine for destination-specific guidance |
| Rabies (Pre-exposure) | Veterinarians, wildlife handlers, lab workers | 3-dose series over 3-4 weeks | Post-exposure prophylaxis very different; may be lifesaving |
| Japanese Encephalitis | Travel to endemic areas; extended stay in high-risk season | 2-dose series | Consider based on specific travel itinerary |
Immunization Documentation
Always document vaccine name, date, lot number, injection site, and manufacturer. Verify immunity status with serology when indicated. Maintain accurate records and provide patients with documentation for their records.
Screening for Common Conditions
Cardiovascular Risk Assessment
For primary prevention, calculate 10-year atherosclerotic cardiovascular disease (ASCVD) risk using validated tools. Discuss statin therapy, lifestyle modification, and blood pressure targets.
10-Year ASCVD Risk Calculator
Use pooled cohort equation or Framingham risk score: - Low risk (<5%): Lifestyle modification, no statin - Borderline (5-7.5%): Consider statin based on shared decision-making - Intermediate (7.5-20%): Moderate- to high-intensity statin - High risk (>20%): High-intensity statin + aggressive BP/lifestyle management
Cognitive Impairment Screening
Cognitive decline in older adults warrants formal assessment. Brief Cognitive Impairment Screen (BCIS) or Montreal Cognitive Assessment (MoCA) identify mild cognitive impairment requiring further evaluation.
Vision and Hearing Assessment
Age-appropriate vision and hearing screening identify modifiable causes of functional limitation. Refer for audiology and ophthalmology as indicated. Hearing aids and glasses significantly improve quality of life and fall risk.
ICU Pearls: Ventilation, Shock, and Code Management
Intensive care medicine demands rapid decision-making, understanding of complex pathophysiology, and familiarity with invasive procedures. This section provides essential frameworks for managing the critically ill.
Mechanical Ventilation Essentials
Mechanical ventilation provides respiratory support when natural breathing cannot sustain adequate oxygenation and ventilation. Understanding indications, modes, and management prevents complications.
Indications for Mechanical Ventilation
When to Intubate and Ventilate
- Respiratory failure: PaO2 <60 mmHg on supplemental oxygen; PaCO2 >50 mmHg with acidemia
- Airway protection: Inability to protect airway (altered mental status, absent gag reflex, aspiration risk)
- Anticipated clinical deterioration: Impending respiratory failure; cannot safely monitor airway
- Shock states: Severe sepsis/shock requiring sedation and airway security
- Procedure-related: Elective intubation for anticipated airway compromise
Ventilator Modes
| Mode | Patient Control | Mechanism | Use Case |
|---|---|---|---|
| AC/VC (Assist Control, Volume Control) | Partially controlled | Clinician sets rate and tidal volume; patient can trigger additional breaths | Most common initial mode; ensures minimum minute ventilation |
| AC/PC (Assist Control, Pressure Control) | Partially controlled | Clinician sets rate and inspiratory pressure; volume varies with compliance | Better for stiff lungs (ARDS); prevents excessive tidal volumes |
| SIMV (Synchronized Intermittent Mandatory Ventilation) | Shared control | Set rate delivered; patient can breathe spontaneously between mandatory breaths | Transition mode during weaning |
| PSV (Pressure Support Ventilation) | Patient-controlled | Patient triggers all breaths; each augmented to preset pressure | Spontaneous breathing trial; used during weaning |
| CPAP (Continuous Positive Airway Pressure) | Patient-controlled | Continuous positive pressure throughout respiratory cycle; patient breathes spontaneously | Non-invasive respiratory support |
| Bilevel (BiPAP) | Patient-controlled | Two pressure levels cycle; patient breathes spontaneously | Non-invasive support for hypoxemia/hypercapnia |
Initial Ventilator Settings
ARDSNet Protocol (Most Restrictive/Protective)
- Tidal Volume: 6 mL/kg of ideal body weight (not actual weight)
- Respiratory Rate: 14-18 breaths/min
- FiO2: Start 100%, titrate to maintain oxygen saturation 88-95%
- PEEP: 5-8 cm H₂O initially; titrate based on oxygenation
- Plateau Pressure: Target <30 cm H₂O (check by inspiratory hold at end-inspiration)
- pH Target: Permit permissive hypercapnia (pH 7.15-7.25) to maintain low tidal volumes
Ventilator Alarms and Troubleshooting
| Alarm | Causes | Management |
|---|---|---|
| High Pressure Alarm | Tube obstruction/kinking, patient biting tube, bronchospasm, secretions, pneumothorax, patient-ventilator dyssynchrony | Auscultate; suction; assess tube position (CXR); manual bagging; check breath sounds |
| Low Pressure Alarm | Circuit disconnect, cuff leak, inadequate PEEP | Check all connections; inspect cuff; verify PEEP setting; auscultate |
| Apnea Alarm | Patient not triggering breaths (apnea or oversedation), trigger sensitivity too high | Assess level of consciousness; check trigger setting; manually ventilate if concerned |
Sedation Management
Sedation Goals in Critical Illness
- Target RASS (Richmond Agitation-Sedation Scale): -2 to 0 (light sedation, arousable)
- Daily interruption: Spontaneous awakening trial daily if no contraindications
- Common agents:
- Propofol: Rapid onset/offset; causes hypotension; useful for rapid sequence intubation recovery
- Dexmedetomidine: Maintains cognition; less respiratory depression; preserves airway reflexes
- Benzodiazepines: Lorazepam for intermediate sedation; midazolam for rapid sedation
Mechanical Ventilation Weaning
Weaning begins when the underlying cause of respiratory failure has improved. Systematic assessment prevents premature extubation and unnecessary prolonged ventilation.
Spontaneous Breathing Trial (SBT) Protocol
- Readiness Criteria:
- Oxygenation: FiO2 ≤0.5; PEEP ≤5 cm H₂O; PaO2 ≥60 mmHg
- Ventilation: No fever; acceptable minute ventilation
- Strength: Spontaneous respiratory effort; negative inspiratory force more negative than -20 cm H₂O
- Trial Method: Switch to PSV of 5 cm H₂O or T-piece for 30-120 minutes
- Success Criteria:
- RR <35 breaths/min; no accessory muscle use
- No hypoxemia (SpO2 ≥90-92%)
- No significant tachycardia; minimal anxiety
- RSBI (Rapid Shallow Breathing Index): RR/TV (in liters). RSBI <105 predicts successful extubation
- Extubation: If trial tolerated well; confirm cuff leak (remove tape, suction above cuff, listen for air leak)
ARDS Definition and Management
Acute Respiratory Distress Syndrome (ARDS) represents severe hypoxemic respiratory failure with bilateral opacities not fully explained by cardiac causes.
Berlin Definition of ARDS
- Timing: Acute onset (within 1 week of known clinical insult)
- Bilateral Opacities: Bilateral infiltrates on imaging not fully explained by effusion, atelectasis, or nodules
- Not Cardiogenic: Respiratory failure not fully explained by cardiac failure or fluid overload
- PaO2/FiO2 Ratio (calculated at minimum PEEP 5):
- Mild: 200-300
- Moderate: 100-200
- Severe: <100
- Management: Low tidal volume ventilation (6 mL/kg), plateau pressure <30, permissive hypercapnia, lung recruitment as needed
Shock and Vasopressor Management
Shock represents inadequate tissue perfusion despite adequate circulating volume. Classification guides therapeutics.
Types of Shock: Hemodynamic Profile
| Type | CVP | PCWP | Cardiac Output | SVR | Primary Problem | Examples |
|---|---|---|---|---|---|---|
| Hypovolemic | ↓Low | ↓Low | ↓Low | ↑High | Inadequate intravascular volume | Hemorrhage, burns, dehydration |
| Cardiogenic | ↑High | ↑High | ↓Low | ↑High | Decreased cardiac contractility | MI, acute HF, cardiomyopathy |
| Distributive (Septic) | ↓Low | ↓Low | ↑High (initially) | ↓Low | Peripheral vasodilation, maldistribution | Sepsis, anaphylaxis, neurogenic |
| Obstructive | ↑High | Variable | ↓Low | ↑High | Mechanical obstruction to flow | PE, tension PTX, tamponade |
Vasopressors and Inotropes
| Agent | Dose | Mechanism | Primary Use | Key Consideration |
|---|---|---|---|---|
| Norepinephrine (Levophed) | 0.1-2 mcg/kg/min IV | α1 > β1 activity | 1st line septic shock; maintains BP while increasing CO | Increased tachycardia and ischemic risk at high doses |
| Vasopressin | 0.04 U/min fixed dose IV | V1 receptor activation | Adjunctive agent in septic shock (combined with NE) | Non-titratable; increases gut vasoconstriction |
| Epinephrine | 0.01-0.5 mcg/kg/min IV | α1 + β1 + β2 activity | Anaphylaxis, cardiac arrest, refractory shock | Metabolic side effects (hyperglycemia, lactate); use as add-on to NE |
| Phenylephrine (Neosynephrine) | 0.5-9 mcg/kg/min IV | Pure α1 activity | Neurogenic shock, acute severe hypertension | Pure vasoconstriction; no inotropic support; may reflex bradycardia |
| Dopamine | 2-20 mcg/kg/min IV | Dose-dependent: low=dopaminergic (renal), mid=β1, high=α1 | Historically common; now less favored in sepsis | Increased arrhythmia risk vs NE; avoid if possible |
| Dobutamine | 2-20 mcg/kg/min IV | β1 > β2 activity; inotrope + mild vasodilator | Cardiogenic shock, acute decompensated HF | Causes systemic vasodilation; monitor BP; use with vasopressor |
| Milrinone | 0.125-0.75 mcg/kg/min IV | PDE3 inhibitor; inodilator | Cardiogenic shock/acute HF with elevated SVR | Hypotension common; no catecholamine effect |
Septic Shock Management Algorithm
- Aggressive IV fluid resuscitation (30 mL/kg crystalloid)
- Source control (antibiotics, drainage, removal of source)
- Norepinephrine if hypotension persists (goal MAP ≥65 mmHg)
- Add vasopressin if additional blood pressure support needed
- Low-dose hydrocortisone if refractory shock
Central Line Placement
Central venous catheters provide access for vasopressor infusion, hemodynamic monitoring, and challenging peripheral access.
Indications
- Vasopressor infusion (mandatory for NE, Epi, Dopa)
- Hemodynamic monitoring (CVP measurement, advanced monitoring)
- Total parenteral nutrition (TPN)
- Difficult peripheral access
- Hemodialysis
- Pulmonary artery catheter placement
Common Sites
| Site | Approach | Advantages | Disadvantages |
|---|---|---|---|
| Internal Jugular (IJ) | Percutaneous puncture; anterior or posterior approach | Reliable landmarks; high success; easy to stabilize | Ipsilateral IJ occlusion risk; positioning challenges |
| Subclavian | Percutaneous puncture below clavicle | Best for long-term use; mobility; low infection | Pneumothorax risk; mechanical complications; positional changes |
| Femoral | Percutaneous puncture below inguinal ligament | Easy access; no respiratory complications | Mobility limitations; DVT/infection risk; backup approach |
Complications
Central Line Complications
- Mechanical: Pneumothorax, hemothorax, arterial puncture (especially femoral)
- Infectious: Catheter-related bloodstream infection (CLABSI); follow bundle approach for prevention
- Thrombotic: Vein thrombosis; phlebitis
- Cardiac: Arrhythmia, right atrial perforation (rare with proper placement)
- Air Embolism: Rare; catastrophic if occurs
- Prevention: Sterile technique, ultrasound guidance, CXR confirmation, prompt removal when no longer needed
Placement Confirmation
Always obtain chest X-ray after central line placement. Confirm catheter tip at junction of superior vena cava and right atrium (not in right ventricle or pulmonary artery). Rule out pneumothorax and hemothorax.
Intubation Essentials
Rapid sequence intubation (RSI) provides safe airway management in emergency/critical settings.
Pre-oxygenation
Pre-oxygenate all patients before intubation attempt to maximize oxygen stores and extend apneic period. Use non-rebreather mask, nasal cannula, or bag-mask ventilation for 3 minutes or 8 vital capacity breaths.
RSI Drugs
| Drug | Dose | Mechanism | Advantage | Disadvantage |
|---|---|---|---|---|
| Etomidate | 0.3 mg/kg IV | GABA agonist; sedative hypnotic | Minimal hemodynamic effect; maintains airway reflexes | Single dose suppresses cortisol; adrenal insufficiency concern |
| Ketamine | 1-2 mg/kg IV | NMDA antagonist | Maintains BP, respiration, airway reflexes; analgesia | Tachycardia, increased ICP; emergence reactions |
| Propofol | 1-2.5 mg/kg IV | GABA agonist | Rapid onset/offset; anticonvulsant | Significant hypotension; bradycardia |
| Rocuronium (Paralytic) | 1 mg/kg IV | Non-depolarizing agent | Fast onset (60-90 seconds); intermediate duration | Rapid sequence gives 6-10 minutes paralysis |
| Succinylcholine (Paralytic) | 1-1.5 mg/kg IV | Depolarizing agent | Extremely rapid onset (30-40 seconds); brief duration | Hyperkalemia risk; malignant hyperthermia; rhabdomyolysis |
Intubation Confirmation
After intubation, confirm tube placement through multiple methods: - Primary: End-tidal CO₂ detection (waveform capnography, colorimetric) - Secondary: Bilateral breath sounds; epigastrium auscultation (no air); CXR
Intubation Complications
- Esophageal intubation: False placement; identified by absent ETCO₂, absent breath sounds
- Right mainstem intubation: Common; confirmed by CXR; withdraw tube slightly (19-21 cm at teeth)
- Dental/lip trauma: Poor technique; can require maxillofacial surgery
- Aspiration: Improper positioning; NPO status; RSI with cricoid pressure
Code Management and ACLS
Cardiac arrest demands rapid, coordinated response. Advanced Cardiac Life Support (ACLS) algorithms guide management.
ACLS Algorithms
VF/Pulseless VT
Ventricular Fibrillation / Pulseless Ventricular Tachycardia Algorithm
- Immediate: Start CPR; attach monitor/defibrillator
- Defibrillate: Deliver one shock (360 J biphasic or equivalent)
- Drug Administration (after first shock):
- Epinephrine 1 mg IV/IO push; repeat q3-5min during cardiac arrest
- Alternative: Vasopressin 40 U IV (single dose, not repeated)
- Rhythm Check: After 2 minutes of CPR, recheck rhythm
- Antiarrhythmics (if VF/pVT persists after 3-5 min):
- Amiodarone 300 mg IV, then 150 mg after 3-5 min; or
- Lidocaine 1-1.5 mg/kg IV, then 0.5-0.75 mg/kg q5-10min (max 3 mg/kg)
- Reversible Causes: Identify and treat H's and T's
- Continue CPR with rhythm checks q2min until ROSC or decision to terminate
Pulseless Electrical Activity (PEA) / Asystole
PEA/Asystole Algorithm
- Immediate: Start CPR immediately
- Epinephrine 1 mg IV/IO; repeat q3-5min
- Consider reversible causes: Treat H's and T's aggressively
- No defibrillation: Neither rhythm responds to shock
- Continue CPR until ROSC achieved or termination decision
Reversible Causes of Cardiac Arrest: H's and T's
| H's (Hypoxia, Hypovolemia, Hydrogen ion, Hypo/Hyperkalemia, Hypothermia) | T's (Tension PTX, Tamponade, Toxins, Thrombosis, Trauma) |
|---|---|
| Hypoxia: Verify airway patency; oxygenate/ventilate; consider intubation | Tension pneumothorax: Needle decompression; tube thoracostomy |
| Hypovolemia: IV fluids; massive transfusion protocol if hemorrhagic | Tamponade: Pericardiocentesis; surgical drainage |
| Hydrogen ion (Acidosis): Effective CPR generates CO₂; avoid sodium bicarb unless specific toxins | Toxins: Identify substance; specific antidotes (naloxone for opioids, cyanide kit, etc.) |
| Hypokalemia/Hyperkalemia: Check serum K+; treat arrhythmias (calcium for K+>7) | Thrombosis (PE): Consider thrombolytics or extracorporeal CPR |
| Hypothermia: Slow, controlled rewarming; extracorporeal techniques for severe cases | Trauma: Ongoing hemorrhage control; consider REBOA, resuscitative hysterotomy |
Post-ROSC Management
After return of spontaneous circulation (ROSC):
Post-Resuscitation Care
- Targeted Temperature Management: Induce therapeutic hypothermia (32-36°C) or at minimum avoid fever
- Coronary Angiography: Obtain 12-lead EKG immediately; cardiac catheterization for STEMI
- Oxygenation/Ventilation: Avoid hyperoxia; target SpO₂ 90-99%; avoid hypocapnia
- Hemodynamics: Vasopressor support, inotropes as needed; maintain MAP ≥65 mmHg
- Prognostication: Neurologic assessment at 72 hours; consider EEG; avoid early withdrawal of care
- Rehabilitation: ICU management; ICU delirium management; early mobility when feasible
Procedure Essentials
Thoracentesis
Fluid drainage from pleural space relieves dyspnea and allows diagnostic analysis. Contraindications include uncontrolled bleeding, small volume (<2 cm), and patient refusal.
Technique: Ultrasound guidance preferred. Insert needle at top of rib (avoid neurovascular bundle running below rib); aspirate fluid for analysis and drain therapeutically.
Paracentesis
Removes ascitic fluid diagnostically or therapeutically. Risk of spontaneous bacterial peritonitis; prophylactic antibiotics if albumin <1.5 or bilirubin >3 in cirrhosis.
Technique: Ultrasound guidance. Local anesthesia. Insert below level of umbilicus to avoid bladder; withdraw fluid slowly.
Lumbar Puncture
Diagnostic testing for meningitis, encephalitis, subarachnoid hemorrhage. Contraindicated in papilledema (risk of herniation). Obtain CT before LP if any mass effect concern.
Technique: Lateral decubitus position; palpate iliac crests (L4 interspace); sterile technique; withdraw CSF and measure opening pressure.
Complications of Procedures
- Thoracentesis: Pneumothorax, hemothorax, organ perforation, infection
- Paracentesis: Peritonitis, bowel perforation, hemorrhage, hepatic/renal failure
- Lumbar Puncture: Post-LP headache (positional), meningitis, spinal cord injury
Resources
Download PDF Version
Clinical Decision Support
- UpToDate — Evidence-based clinical decision support with treatment recommendations at the point of care.
- Open Evidence — AI-powered platform that synthesizes peer-reviewed medical literature for evidence-based decisions.
- Amboss — Medical knowledge library with integrated clinical decision support, drug references, and board review.
- DynaMed — Evidence-based clinical reference with systematic literature surveillance and expert analysis.
Calculators & Scoring Tools
- MDCalc — Validated clinical decision tools, risk scores, and diagnostic calculators.
- ClinCalc — Drug dosing calculators, pharmacokinetic tools, and clinical equations.
Drug & Antimicrobial References
- Sanford Guide — Comprehensive antimicrobial therapy reference with evidence-based recommendations for antibiotic selection and dosing.
- Lexicomp — Drug information database with dosing, interactions, and patient education.
Specialty References
- Life in the Fast Lane (LITFL) — Emergency medicine and critical care education with an excellent ECG library.
- EMCrit — Critical care and emergency medicine blog with evidence-based protocols and podcast.
- Radiopaedia — Free collaborative radiology reference with imaging cases and articles.
- CoreIM — Internal medicine podcast covering high-yield clinical topics with visual aids.
- Time of Care — Common work-up orders for inpatient and outpatient medical conditions.
Board Review & Education
- MKSAP 20 — American College of Physicians' medical knowledge self-assessment program for board preparation and CME.
- University of Chicago Housestaff Guide — Reference for critical care, heme/onc, and procedures.
- MGH Whitebook 2024-2025 — Massachusetts General Hospital house officer handbook.
Bibliographic References
- Internal Medicine Survival Guide — HCA Healthcare, RRMC Internal Medicine. Author: Jessica White, DO. Contributors: Bryan Le, DO; Lisa Crabtree, DO. Review Committee: Asif Shah, MD; Kunal Patel, MD; John O. Pittman, MD; Megan White, DO.
- University of Colorado Intern Survival Guide
- Brown University Internal Medicine Intern Survival Guide and orientation materials
- Washington Manual Internship Survival Guide
- UIC Critical Care Guide
- Kenzie Daniels' Intern Survival Guide
- Your Practical Survival Guide to Surgical Internship (Derek F. Amanatullah, MD, PhD, Department of Orthopedic Surgery, University of California Davis Medical Center)
- Podolsky A, Stern DT, Peccoralo L. The Courteous Consult: A CONSULT Card and Training to Improve Resident Consults. J Grad Med Educ. 2015;7(1):113-7. doi: 10.4300/JGME-D-14-00207.1. PMID: 26217436; PMCID: PMC4507900.
Contribute
If you are interested in contributing please contact the SGMC IM Resident Guide team.

Samuel Edusa, MD
For questions, concerns, suggestions, or technical difficulties you may contact samuel.edusa@sgmc.org.

Rosaida Silverio Lopez, MD
For questions, concerns or suggestions contact
rosaida.silverio@sgmc.org
Original guide compiled by Dr. Silverio Lopez

Ornob Rahman, MD
For questions, concerns or suggestions contact
ornob.rahman@sgmc.org
Rotations
Night medicine
Night Medicine Guide
Night Medicine Guide
Purpose
The Graduate Medical Education Night Medicine Guide provides a framework for GME faculty, residents, and other stakeholders to ensure an effective, safe and efficient learning environment in accordance with ACGME requirements.
Introduction
Night medicine offers residents a unique experience in patient care which involves safe transitions of care, admissions, and exposure to the management of emergent and urgent issues that may occur with patients admitted to teaching service.
In light of the fact that the transition to a teaching service has occurred before our residents becoming seasoned PGY3's the workflow will have to be determined by resident milestone expectations and competence keeping the safety of our patients as a priority.
- Supervised admissions will prioritize clinic patients. Program will safely institute a progressive increase in volume, complexity and resident responsibility with regards to patients assigned as senior residents become more competent to the end of academic year.
- If a non-faculty member works for teaching service on a Call day, expectation will be to staff morning and evening admissions and be available for urgent calls overnight.
- Goal admissions or maximum encounters per night (for one PGY1 with one PGY 2 or 3 Team) is 6 patients. For only single PGY 2 or 3 on nights where schedule demands, maximum encounters is 3 patients. Clinic flex of additional 1-2 admissions will not apply to single resident on nights.
Team Structure
1 PGY2 or 1 PGY3 with PGY1
Procedure
- I. Night Medicine team will attend sign-out which is protected time from 7-7.30am and 7-7.30p. Unstable patients will be prioritized.
- II. Night Medicine Team will take floor calls and respond to all urgent bedside needs for Teaching Service patients.
- III. Night Medicine Team will be provided with guidelines regarding timely communication with Supervising Attending.
- IV. Night Medicine Attending will provide supervision for admissions, feedback, and relevant educational teaching points for learning.
- V. Night medicine Team will be expected to attend all codes and rapids to enrich learning experience with the expectation of leading these scenarios when teaching service patients are involved.
Specific Roles and Responsibilities
Supervising Faculty (Night Medicine Attending)
Supervising Faculty is expected to:
- Review all H&Ps and give feedback on improving documentation
- Provide feedback to the night learners performing at least one history and physical per night and give feedback for improvement
- Provide the Intern/resident with the opportunity to practice oral presentation skills and give appropriate feedback at Wednesday Morning reports scheduled for night team.
- Supervise the resident in developing patient care plan for all admitted patients
- Be available to resident at all times by phone to answer questions
- It is the faculty member's responsibility to review goals and objectives, appropriate methods and when to call supervisor with the intern at the beginning of the rotation or shift change.
- Verbal and written feedback is expected from the supervisor, evaluations will be sent through New Innovations system.
Learners
- Residents are expected to contact their supervising Faculty after completion of review of their assigned patients to discuss their evaluation and plan of care.
- Residents will be responsible for appropriate hand off of new and cross coverage patients to the ward teams in the morning.
- Residents are expected to contact their supervising Faculty in the event of patient death.
- Residents are expected to contact their supervising Faculty if patient signs out against medical advice.
- Residents are expected to contact their supervising Faculty if patients Code Status changes.
- Residents are expected to contact their supervising Faculty if patient is transferred to higher level of care.
- Residents are expected to contact their supervising Faculty if patient is anticipated to become acutely unstable or in extremis or with acute decompensation.
Patient Distribution
- Overnight admissions will be added to call Teams list till 7am.
- If Call team is capped before 7am then admissions will go to Pre-Call Team.
Night Team Admission Requirements/Criteria
To help facilitate appropriate patient care and maintain safety standards these guidelines will assist night team / ED providers to determine patients appropriate for night admission.
- Guidelines dictate the appropriate level of care for Night Team should be med/surg and step down (SDU) patients with great probability for improvement overnight with appropriate medical interventions.
- Please ensure that all admissions have appropriate consult service required on call before accepting admission, especially in the case of Urology, ENT
- Please ensure that complex patients do not need to transfer to Tertiary center before admission order placed.
Specific Examples of Appropriate Patients For Nighttime Admission
- Acute MI /Acute Coronary Syndromes with appropriate consult established in the ED
- Cardiac rhythm abnormalities requiring monitoring in SDU with stable hemodynamics
- Hypertensive emergency patient requiring IV antihypertensive and monitoring in the SDU
- Acute hypercapnic respiratory failure with clinical improvement displayed in the ED on BiPAP therapy and PH >7.2, PCO2 <70
- Acute gastrointestinal bleeding but hemodynamically stable and needing frequent hemoglobin checks and monitoring for rebleeding
- Severe Sepsis not requiring pressor support or fluid responsive
- Congestive heart failure exacerbations with significant oxygen requirement without need for vasoactive drips (Dobutamine/ Milrinone)
- *Diabetic Ketoacidosis (Exception to ICU level of care)
Specific Examples of Inappropriate Patients for Nighttime Admission
- Requiring continuous hemodynamic monitoring / On vasoactive agents
- Intubated on mechanical ventilation
- Requiring invasive hemodynamic monitoring, including pulmonary artery catheters, arterial catheters, and circulatory assist devices such as Impella.
- Temporary pacing
- Sudden cardiac death s/p ROSC
- Acute intracranial bleed requiring ICU monitoring, and Hypertonic Saline therapy
- Septic Shock requiring pressor support
- New Acute renal failure not amenable to medical management and likely to require renal replacement therapy
- Pulmonary embolism with hemodynamic instability, and who may require thrombolytic therapy
PCP Admission Exclusion List
If the patient being admitted has any of the following PCPs listed below DO NOT ADMIT. The Apogee hospitalist will do the admission.
PCP Admission Exclusion List
List of PCPs whose patients we do not admit:
- Dr. Larry Smith
- Dr John Anderson
- Dr. Bennett Hogan
- Dr. Brian Griner
- Dr. Lyn Lee
- Dr. Seth Courson
Outpatient Ambulatory
Resident Continuity Clinic Expectations
Resident Continuity Clinic Expectations
Internal medicine specialists should have the skills necessary to manage virtually any adult medical problem. As internists, we gain experience through rigorous training during residency, including subspecialty rotations, to handle complex issues. In the ambulatory setting, preventative medicine with a focus on evidence-based guideline driven care is essential.
During your continuity clinic ambulatory experience, you're going to learn how to take care of many common and complex problems, perform outpatient procedures, and manage things that many clinics would have sent to a specialist. You'll learn, through a patient-centered and problem-driven approach, how to cost-effectively manage virtually every adult medical problem in a safe, effective, and guideline-driven manner. Your patient care will be coordinated with a board-certified internist who will provide mentorship, directly supervise, and guide you through a graduated level of autonomy and increasing responsibilities that prepares you to practice independently by the time you complete your residency.
A Typical Day in Clinic
Morning Clinic
- Arrive at 8 am. It's important that you get here before patients arrive so that you can review any labs, imaging, or inbox items from the previous day. This is a good time to pour a cup of coffee and handle any outstanding items, so they don't bog you down during the day.
- First patient at 8:30 am. This may be a scheduled follow-up or a work-in for an urgent problem visit. You won't always have an 8:30 am patient, and this could even happen at the last minute from a walk-in request.
- Last patient during morning ½ day block is scheduled at 11 am. Since conference starts after noon, this gives you an hour to evaluate, manage, staff and hopefully write the note for your last patient of the morning.
- You're doing wonderful if you're able to see all of your patients and write all of your notes before going to conference, though most people won't be able to write many (or any) notes before going to conference - especially at first. Don't worry, you'll get faster before you know it.
Afternoon Clinic
- Arrive for your first patient by 1:30 pm. Last patient is scheduled no later than 4 pm. Clinic closes at 5 pm and office staff leaves.
- Interns and residents are typically in clinic until about 5:30 pm finishing up notes and ensuring that patient calls and inbox items are caught up prior to going home. You can certainly go home sooner, e.g. after the last patient in the clinic has been seen, if all your clinic work is done.
- Pro-tip! Don't take your work home with you. It's healthiest and best for your well-being to keep all work at work. All notes from the clinic must be completed on the same day.
Note
PGY-2 and PGY-3 Have Different Schedules and Expectations
As you would expect, an intern has a lot to learn about the flow of the clinic, ambulatory medicine, how to write notes, require longer times to staff patients, and have most of the responsibility of establishing care with new patients. Interns are going to see fewer patients, and as fund of knowledge and experience increases, you will attain a graduated level of responsibility and autonomy. As you master the common problems, patient volume is essential - allowing you to see rarer or unique conditions that allow for learning and growth. The goal is to see these numbers of patient encounters, and this often requires scheduling more patients with the anticipation of cancellations and no-shows.
PGY-1
- First half of academic year: 3-4 patients per ½ day
- Second half of academic year: 4-5 patients per ½ day
PGY-2
- First half of academic year: 5-6 patients per ½ day
- Second half of academic year: 6-7 patients per ½ day
PGY-3
- 7-8 patients per ½ day
Note: there are clinic scheduling nuances that affect how and why schedules are built the way they are, and this may not be readily apparent to you. Some schedules are left more open for work-ins, reduced to accommodate more new patients, or increased to accommodate many PCP follow-ups etc. Schedules will not be equitable between PGY years nor even between residents within the same PGY year. Additionally, these numbers may change depending on the number of clinic attendings in office and overall clinic patient load.
Staffing Patients with the Attending
All patients must be staffed with your assigned clinic attending, regardless of complexity or whether here for a new or patient follow-up, during the first six (6) months of intern year. These patients are coded with a "GC" modifier, which signifies to CMS that the attending physician saw and evaluated the patient with you.
After six (6) months of training, at the discretion of your attending and your own comfort level, you may start sending patients home from the clinic without the attending physically going and seeing/staffing that patient. Patients should be discussed with the attending while still in clinic or by the end of the half-day. These patients will be billed with the "GE" modifier to signify a "primary care exception" to direct supervision with CMS. This can only be done at your primary resident continuity clinic. This is to allow professional growth, autonomy, and increased patient volume to see uncommon presentations of common or rare problems, which is necessary to prepare you for independent practice.
Presenting New Patients:
In these visits, we want to be thorough and do a broad review of systems and physical exam. You do not have to present your entire exam, but we do want to "check the boxes" of going over the full medical history.
- Start with the patient's name, age, and reason for establishing care. For example: "Ms. Smith is a 67 y.o. female here to establish care, she was previously followed by Dr. Doe in Miami and just moved here to live with her daughter."
- Next present past medical history and medications together - every med should go with a problem. Follow this with the rest of the past medical history - family, social, surgical, and allergies.
- Note pertinent review of system.
- Physical exam - starting with vitals.
- Assessment and plan - problem based. For example: "For essential hypertension, blood pressure is above goal today at 145/90. They check BP at home and it's about the same. Given their history of diabetes, the ADA recommends a BP goal of 130/80. They do not check ambulatory blood pressure. I gave them a blood pressure log and a printout for the DASH diet, and we agreed to start low-dose amlodipine today."
Presenting Follow-up Patients:
These are problem-based visits and, because patients often have many problems and medications in a residency clinic, we typically only discuss what is being managed today.
- Start with patient's name, age, and reason for today's visit. For example: "Ms. Smith is a 67 y.o. female here for follow-up of hypertension, type 2 diabetes, and stage III obesity."
- Next, present the issues you are going to discuss in a problem-based manner. For example, "For her hypertension: blood pressure is well-controlled on lisinopril 20 mg daily, no cough, lightheadedness, headache, chest pain, dyspnea, orthopnea, or lower extremity edema. Physical exam is unremarkable: vitals normal with BP 120/80, normal heart and lung sounds with no peripheral edema. I'll refill her medication without any changes and check a metabolic panel for renal function and potassium since she hasn't had labs in a year" ... Repeat for other problems.
- "We will have patient follow-up in 3 months for hypertension, etc."
Patient Requests for a Specific Attending
Background: many of the patients at our teaching clinic were originally managed by our teaching attendings, and these patients were transitioned to resident PCPs. Some of these patients will ask to see a specific attending and, if they ask, you should staff that patient with the attending they requested, along with any orders and the note to co-sign.
Scheduling Patient Follow-ups
The two most important aspects of a patient follow-up: 1. Continuity between a patient and their primary care physician 2. Timing of the follow-up
A few tips for determining the appropriate patient follow-up date
- Most important tip - know your schedule. You want to ensure your patients are following up with you unless it's unavoidable.
- Don't knee-jerk to a routine 3-month follow-up. Consider, generically, the following situations:
- Uncontrolled hypertension? 2-4 weeks
- Uncontrolled anxiety or depression? 2-6 weeks
- Severe new pain? 1-2 weeks
- Acute on chronic heart failure? 3-14 days
- Cellulitis? 1 week
- Well-controlled diabetes for a long time and no recent med changes? 4-6 months
- Routine 3-month follow-up but you are only in clinic 2 months from now and again 5 months from now? Consider making it a 5-month follow-up
- You really need the patient to be seen again in 2 weeks and you only have an appointment 2 months from now? Look at the schedule with the front desk, find a resident with an available appointment, and call the resident who will be seeing them to sign-out your patient and plan
Writing Notes
We use smart phrases that generate an H&P and progress note template. We prefer everyone to use the same template so that all notes look similar. Your clinic attending or upper-level resident can help you acquire these templates if they're not already added to your clinic build. Note that you want to be in the "SGA Internal Med Park" Epic context for these to show up in a clinic-driven format. If you're coming from the hospital, you may be in a hospitalist context which simply customizes your build for things like autogenerating notes or billing based on where you're at.
Billing
Billing can be nuanced and complex, even for the best physicians. You don't have to be an expert at billing and, even if you were, billing rules are likely to change by the time you graduate anyways. You'll learn much about billing during your 3rd year of residency, until then the basics will suffice. Ultimately, your attending is the "billing provider"; however, your role is to choose what you think the appropriate billing is prior to closing your encounter.
- 99213: Low complexity (level 3) follow-up. This would be appropriate for an acute, uncomplicated illness that doesn't require treatment or just something over the counter - like viral pharyngitis. This also implies that you didn't discuss or address any other medical issues.
- 99214: Moderate complexity (level 4) follow-up. Probably 90% of all your follow-up encounters will be at level 4. While this can get technical, an easy way to reach this billing level is addressing two chronic problems and one prescription medication. For example, continuing metformin for type 2 diabetes and encouraging weight loss for obesity will qualify for a level 4 follow-up.
- 99215: High complexity (level 5) follow-up. You pretty much have to be dealing with a life-threatening illness and consider sending them to the hospital or emergency department to reach this billing code.
- New visits and time-based billing: New patient visits are billed the same, other than codes are 99203, 99204, 99205. Attending physicians can also bill on time, but it must be their time - not yours.
- Billing procedures: these are usually done by using a "25" modifier to add on a "significant, separate event" like a Medicare annual wellness, skin biopsy, joint injection, etc. We prefer a separate note for these things, and there are smart phrases in Epic we can get you to make this easy to document.
Managing Your Patient Phone Calls
You care for a panel of patients. You are their primary care physician. They may call to ask questions about your management, a medication you prescribed at their last appointment, get a medication refilled, get prior authorization letter written, etc. Sometimes the front desk staff or residents in clinic can help you with these, but ultimately your patients are your responsibility. This is part of the continuity of care that we train you for, and this continuity is an expectation of the ACME, your residency accrediting body. These messages will be sent to you, and regardless of your rotation you hold responsibility for ensuring that they are handled. Be diligent and ensure things that get sent to your inbox get handled, regardless of where your rotation is at the time.
Managing Your Inbox and Result Notes
Any labs, imaging orders, or other inbox messages should be managed promptly. For critical results, this is 24 hours (or sooner if is potentially life-threatening). Patient phone calls should be handled preferably same-day, within 24 hours. For routine abnormal results, patients should be notified within 7 days. You have several options for managing this:
- Send results via MyChart through a result note. Be sure to write an assessment (what is going on), plan (what you're doing about it), and contact (how you let the patient know). Be sure the patient checks their MyChart before using this method, which can be done easily in Epic. Avoid sending MyChart notes for significant medical diagnosis or time-sensitive issues.
- Write a result note and send it to the front desk to call for you. This is great for when patients don't have MyChart or you want to ensure they get a phone call from a nurse to know about a medication change etc. This is also a great way to reach the patient if you're writing a result note while on nights or the weekend.
- Call the patient yourself. For example, an abnormal breast MRI or new diagnosis of osteoporosis or diabetes would be best discussed over the phone or calling the patient into the office for an appointment - depending on circumstances.
- Ask the front desk to schedule an appointment to discuss abnormal results. Sometimes you need a long time to talk about management options and prognosis - do this in a clinic appointment if necessary.
Note: ignoring or delaying test results, phone calls, and medication refills from your patients is unprofessional, and it is harmful to the patient-physician relationship. Your clinic attending is always available to help you manage these results and patient calls should you have questions or are unsure. Documenting that you addressed these items is imperative.
Disciplinary Actions
Your ability to responsibly manage your patients is a cornerstone of your professionalism evaluation, and failure to meet expectations will result in disciplinary action at the program level. Corrective actions will be commensurate with the infraction. Most corrective actions start with verbal or informal feedback, followed by formative feedback which may or may not be in writing, and can escalate to written feedback and referral to the program director. Any of these methods of feedback are referrable to the clinical competency committee and the program director to be addressed during your semi-annual or annual evaluations. Corrective action may include remediation, probation, suspension, up to dismissal from the program.
Availability to Clinic Staff and Colleagues
Please remain in the resident workroom during office hours while in the clinic. This space is available to the front desk staff, and remaining with your other residents allows for mentoring and helping opportunities. Please refrain from using any attending physician back offices, which takes you away from your colleagues, and there may be sensitive items on the computers or in desks.
Additionally, we use Microsoft Teams for in-clinic communication. Please have this active on your work computer and/or cellphone while in the clinic. The lab or scheduling desk, for example, may have a question about an order or when to follow-up if not clear.
Dot System in Epic
You will notice colored dots next to patients' names in the clinic. This replaces the old-school way of doing things, like putting flags outside the room or lights that communicate ready status. These colors are semi-automated:
- Green: once the patient is checked in and triage has obtained vitals, med rec, assisted with adding setting up care gap orders and refills, etc. - they are put in a room and marked ready for you to see them. "Green for GO!"
- Blue: if a lab order, POCT, etc. is placed, the color will change to blue which signifies for the lab to get the patient. You may want to wait to sign all orders at the end of the visit so that the lab doesn't interrupt you, unless that's what you want (for a fingerstick A1c etc.)
- Black: After your patient leaves the office, please manually change their color to black. This signifies to the attending and staff that the patient should no longer be here.
- There are other colors (red, white) that aren't being used. We may change this in the future.
Vacation Policies
Vacation should be scheduled far enough in advance that you don't inadvertently schedule patients to see you on days you are not in clinic. Patients are entitled to see their primary care physician and should not be shuffled around to see other residents due to poor planning on our part. If you are on nights, vacation, or on some other rotation that will have you missing clinic - be sure there are no patients on your schedule. If your schedule changes unexpectedly - it is your responsibility to ensure that your schedule in the clinic is correct.
If you or on vacation or a leave of absence, you are required to assign your inbox to a partner to manage while you are gone. You must have your inbox (results, refills, calls) caught up and addressed before your last day of work
- Resident Leave Request Form: Download the form here
Evaluations
You'll get a formal evaluation written by your clinic attending after your monthly rotations. You'll also get informal feedback throughout the rotation, either on a case-by-case basis and preferably with a sit-down private meeting part-way through your rotation to discuss how you are performing, areas to improve to get you to the next level, and how to achieve your future goals. Additionally, the ACME expects residents to obtain competency in six core areas prior to graduating. Your feedback will help you achieve these goals.
Revised July 1, 2024
Notes
Hypertension in the clinic
Management of hypertension in the clinic (chalk talk) - Dr. Hayes 07/30/24
Evaluating Blood Pressure
- First step is confirming the patient actually has elevated blood pressure
- Many factors can falsely elevate BP readings:
- Wrong cuff size
- Patient smoking/drinking coffee beforehand
- Full bladder (can raise BP 10-15 points)
- Not resting for 5 minutes before measurement (can raise BP 10-20 points)
- Patient talking during measurement
- Best practice:
- Have patient rest 5 minutes before measurement
- Take BP as last vital sign
- Patient should not talk during measurement
- Use proper cuff size
- Consider having patient empty bladder first
- Implementing these changes led to 8 point drop in systolic and 6 point drop in diastolic BP on average
- Ambulatory BP monitoring gives the most accurate picture of true BP
- Home BP measurements are useful but home devices may not be as accurate
Initial Evaluation
- For new hypertension diagnosis, always order:
- Basic metabolic panel - to check renal function, electrolytes
- EKG - to look for signs of end organ damage
- Look for signs of secondary hypertension:
- Low potassium may indicate hyperaldosteronism
- EKG changes may indicate underlying heart/lung issues
When to Treat
- No specific BP threshold necessitates emergency treatment if asymptomatic
- Symptoms + very high BP (generally >180/110) may indicate hypertensive emergency
- For hypertensive emergencies, lower BP gradually by 25% initially
- Rapid BP lowering in chronic hypertension patients can cause stroke-like symptoms
- For asymptomatic elevated BP, treatment can be initiated over days to weeks
Treatment
- Three main drug classes proven to reduce cardiovascular events:
- Thiazide diuretics (chlorthalidone preferred over HCTZ)
- ACE inhibitors
- Calcium channel blockers (dihydropyridines like amlodipine)
- Choose based on patient characteristics/comorbidities
- Beta blockers not recommended as first-line (may increase heart failure risk)
- Start with 2 drugs if BP >20/10 mmHg above goal
- Goal BP:
- Generally 130/80 for high risk patients (e.g. diabetics)
- 140/90 may be acceptable for low risk patients
- Consider screening for secondary causes if BP uncontrolled on 3+ meds including a diuretic
Other Considerations
- Low salt diet lowers BP but no direct evidence it reduces CV events
- Nocturnal BP control important - consider nighttime dosing of meds
- Once started, BP meds usually need to be continued long-term
- There is no BP that is "too low" as long as organs are perfused and patient is asymptomatic
- Diastolic BP may be more important than systolic for CV risk
References
- The ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. Major Cardiovascular Events in Hypertensive Patients Randomized to Doxazosin vs Chlorthalidone: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA. 2000;283(15):1967–1975. doi:10.1001/jama.283.15.1967
Anxiety & Depression in the clinic
Understanding Anxiety & Depression (chalk talk) - Dr. Hayes 12/05/24
Key points
-
Prevalence & Normalization
- Most people will meet criteria for anxiety/depression at some point
- Particularly high among medical students (estimated ~70%)
- Important to communicate to patients that having anxiety/depression doesn't mean something is wrong with them
- "Only good people get anxiety or depression" - shows they care
-
Adaptive vs. Problematic Anxiety
- Some anxiety is beneficial for motivation
- Too much anxiety can be overwhelming and counterproductive
- Often stems from caring too much about life circumstances/others' perceptions
- Can manifest as physical symptoms
-
Diagnostic Tools & Screening
- GAD (Generalized Anxiety Disorder) Screening:
- GAD-7: Full screening tool with 7 questions
- GAD-2: Quick screening version with 2 key questions:
- Feeling nervous
- Not being able to stop worrying
- Scoring: 0 (never) to 3 (most/all of the time)
- Score >2 on GAD-2 indicates need for full GAD-7
- GAD (Generalized Anxiety Disorder) Screening:
-
Depression Screening:
- PHQ (Personal Health Questionnaire)
- PHQ-2 quick screening questions:
- Feeling down/hopeless/crying
- Loss of interest (anhedonia)
Diagnostic Criteria & Assessment
- Based on DSM-5 (Diagnostic and Statistical Manual, 5th version)
- Key differences between screening tools and DSM criteria:
- GAD requires 6 months of symptoms
- Depression requires 2 weeks of symptoms
- Symptoms must impact daily life/functioning
- Scores can indicate severity (mild, moderate, severe)
- Can track treatment progress using scores
Types of Anxiety
-
Generalized Anxiety Disorder (GAD):
- Chronic, lifetime condition
- May be well-controlled but can flare with stressors
- Requires long-term management
-
Situational Anxiety:
- Temporary, linked to specific circumstances
- May not require long-term medication
- Examples: exam anxiety, medical concerns
-
Anxiety vs. Panic Attacks:
- Anxiety attacks: Have specific triggers/reasons
- Panic attacks: Occur without warning or apparent cause
- Both can have severe physical symptoms
Treatment Options (Three Main Modalities)
-
Exercise:
- Equal efficacy to other treatments
- Increases hippocampal volume
- Can be challenging to initiate when feeling unwell
-
Therapy:
- Various types (CBT, desensitization, etc.)
- Provides lifetime coping tools
- Some patients skeptical of effectiveness
-
Medication:
- SSRIs/SNRIs first-line treatment
- ~30% remission rate for single medication
- Often requires 3 medication/dose changes
- 90% eventual cure rate with persistence
-
Medication Considerations
- First-line options:
- Sertraline
- Fluoxetine
- Escitalopram
- Selection based on side effects and patient preferences
- First-line options:
Special considerations:
- Weight gain concerns: Consider fluoxetine, sertraline, bupropion, venlafaxine
- Sleep issues: Consider TCAs, trazodone, mirtazapine
-
Missed doses: Consider longer half-life medications like fluoxetine
-
Benzodiazepines:
- Limited use, mainly for:
- True panic disorder
- Short-term bridge until SSRIs take effect
- Short-acting (Xanax, Ativan) for occasional use
- Long-acting (Clonazepam, Valium) for all-day anxiety
- Generally safer than opioid dependence
- Use with caution in elderly (>65)
- Limited use, mainly for:
Male Hypogonadism: Clinical Management
Noon Lecture | Richard Bias, MD | 06/05/25
I. Introduction and Scope
Topic Focus: Male hypogonadism (Part 1 of broader hypogonadism series)
Excluded Topics:
- Female hypogonadism
- Transgender medication
- Detailed congenital cases
Clinical Context: Presentation focuses on practical clinic-based approach to diagnosis and management
II. Definition and Classification
Basic Definition (UpToDate)
Decrease in one or both major functions of male gonads:
- Sperm production (spermatogenesis)
- Testosterone production (steroidogenesis)
Primary vs. Secondary Hypogonadism
Primary Hypogonadism (Testicular origin)
- Lab Pattern: ↓ Testosterone + ↑ LH/FSH
- Most Common Cause: Age-related decline
- Mechanism: Direct testicular dysfunction
Secondary Hypogonadism (Hypothalamic-Pituitary origin)
- Lab Pattern: ↓ Testosterone + Normal/↓ LH/FSH
- Mechanism: Inadequate gonadotropin stimulation
III. Etiology
Primary Hypogonadism Causes
Congenital:
- Klinefelter syndrome
- Androgen receptor mutations (androgen insensitivity syndrome)
- Cryptorchidism (if uncorrected)
- Androgen synthesis defects
Acquired:
- Infections (especially mumps orchitis)
- Radiation/chemotherapy
- Opioid use
- Alcohol use disorder
- Androgen blockers (finasteride)
- Testicular trauma/torsion
- Autoimmune damage
Secondary Hypogonadism Causes
Congenital:
- Kallmann syndrome
- Congenital GnRH deficiency
Acquired:
- Pituitary adenomas/tumors
- Hypothalamic dysfunction
- Chronic illness
- Medications
- Obesity
IV. Clinical Presentation and Evaluation
Typical Patient Scenario
48-year-old male presenting with:
- Decreased morning erections
- Reduced libido (from daily thoughts to monthly)
- Partner concerns about sexual interest
Initial Clinical Assessment
Essential History Taking:
- Rule out depression (PHQ-9)
- Assess for sleep apnea
- Evaluate obesity/BMI
- Screen for uncontrolled diabetes
- Review medications
- Sleep hygiene assessment
Key Point: Don't immediately jump to testosterone testing - comprehensive evaluation first
V. Laboratory Testing Protocol
Testosterone Testing Guidelines
Timing Requirements:
- Morning collection: 7-10 AM (8-10 AM in clinic)
- Rationale: Diurnal variation with morning peak
- Two separate tests: Confirm low reading on different days
What to Order:
- Serum total testosterone
- Free testosterone
- LH and FSH (to distinguish primary vs. secondary)
When NOT to Test
Avoid testing during:
- Acute illness (wait 6-8 weeks post-recovery)
- Recent steroid administration (wait 6-8 weeks)
- Immediately post-hospitalization
Reference Ranges - Multiple Guidelines
| Organization | Cutoff (ng/dL) | Notes |
|---|---|---|
| NIH | Age-specific ranges | Preferred approach - accounts for age |
| AUA | <300 | One-size-fits-all |
| UpToDate | 264-916 or lab-specific | Variable by assay |
Clinical Pearl: Treat the patient, not the number. Consider symptoms alongside lab values.
Special Circumstances for Free Testosterone
Order when concerned about binding globulin abnormalities:
- Obesity (mild to severe)
- Advanced age
- Suspected binding protein disorders
VI. Diagnostic Criteria
Requirements for Diagnosis
Both conditions must be met:
- Low testosterone levels (confirmed on two separate occasions)
- Compatible clinical symptoms
Target Symptoms (Evidence-Based)
Primary indication: Sexual dysfunction
- Erectile dysfunction
- Decreased libido
- Reduced morning erections
Non-indications (insufficient evidence):
- Fatigue alone
- "Low energy"
- Cognitive complaints
- General "vitality" concerns
Clinical Reasoning: These non-specific symptoms have multiple etiologies and limited response to testosterone therapy.
VII. Treatment Guidelines
American College of Physicians (ACP) Recommendations
Recommendation 1A:
- Initiate testosterone in men with age-related low testosterone AND sexual dysfunction
- Patient must desire improvement in sexual function
- Discuss benefits, harms, and costs
Recommendation 1B:
- Re-evaluate symptoms at 12 months and periodically thereafter
- Discontinue if no improvement by 12 months
Recommendation 2:
- Do NOT initiate testosterone for:
- Energy/vitality
- Physical function
- Cognition
- General "anti-aging"
Endocrine Society Guidelines (2018)
Evidence supports benefits for:
- Sexual function
- Unexplained anemia (helps counteract polycythemia risk)
- Bone density (especially in older men)
Monitoring requirements:
- Prostate cancer screening discussion
- Cardiovascular risk assessment
VIII. Treatment Modalities and Costs
Available Formulations
| Route | Frequency | Advantages | Disadvantages |
|---|---|---|---|
| IM Injection | Biweekly | Cost-effective, ACP preferred | Peak/trough levels |
| Transdermal Gel | Daily | Steady levels, convenient | Expensive |
| Pellets | 3-4 months | Long-acting | Very expensive, dose inflexibility |
Cost Analysis (2016 data)
- Transdermal gel: ~$2,100/year (Medicare Advantage)
- IM injections: ~$156/year (Medicare Advantage)
- Cost ratio: >13:1 difference
ACP Preference: IM injections due to cost-effectiveness
IX. Contraindications and Precautions
Absolute Contraindications
- Active prostate cancer
- Breast cancer
- Desire for fertility (relative)
Relative Contraindications/Precautions
- Recent MI/stroke: Wait minimum 6 months
- Uncontrolled sleep apnea: Optimize first
- Severe heart failure: Use caution
- High prostate cancer risk: Enhanced monitoring
Prostate Cancer Risk Assessment
High-risk categories:
- Age 40-69 with family history (first-degree relative <55 years)
- African American men
- Age ≥55 (routine screening age)
Key Point: Testosterone does not cause prostate cancer but may accelerate existing undiagnosed cancer.
X. Adverse Effects and Monitoring
Common Adverse Effects
1. Erythrocytosis (most common)
- Monitor hematocrit
- Therapeutic phlebotomy if >52-54%
- Consider 81mg aspirin
2. Sleep apnea worsening
3. Gynecomastia/breast tenderness
4. Acne (face, back, chest)
5. Testicular atrophy (dose and duration dependent)
Fertility Considerations
- Testosterone = male contraception
- Discuss family planning before initiation
- Clomiphene alternative: Preserves fertility and testicular size
- Either/or decision: Not combination therapy
XI. Monitoring Protocol
Baseline Labs (Before Treatment)
- CBC (hematocrit baseline)
- Lipid panel
- PSA (if age ≥55 or high risk)
- LH/FSH (determine primary vs. secondary)
- Total and free testosterone
Follow-up Schedule
- 3 months: Testosterone level, CBC, symptom assessment
- 6 months: PSA (if applicable), full panel
- 12 months: Complete reassessment
- Annually thereafter: If stable and responding
Testosterone Level Timing on Treatment
For injections:
- Peak level: 3-4 days post-injection
- Trough level: Day before next injection
- Clinical decision: Based on symptoms + levels
For gels: - Anytime: Steady-state levels
XII. Prostate Monitoring
Screening Requirements
Age-based:
- 55-69 years: Routine PSA screening
- 40-54 years: Only if high risk
Monitoring on treatment:
- Baseline PSA required
- Follow-up PSA at 6 months, then annually
- Concerning change: >1.2 ng/mL increase from baseline
DRE Controversy
Arguments against routine DRE:
- Limited palpable prostate surface
- Urology will perform anyway
- PSA more objective
Requirements if PSA elevated:
- Repeat PSA (avoid stimulation 1 week prior)
- Urology referral if persistently elevated
- Consider DRE per training/preference
XIII. Dosing Guidelines
Typical Starting Doses
IM Injection:
- Initial: 150mg every 2 weeks
- Adjustments:
- Increase to 200mg biweekly, OR
- Change to 150mg weekly
Transdermal:
- 1% gel: Lower abdomen application
- 1.62% gel: Upper arms/shoulders only
- Dose: Usually 2 pumps daily, adjust based on levels
XIV. Special Considerations
Cardiovascular Effects
- Current evidence: Unclear risk/benefit profile
- Historical concerns: DVT/PE/MI/stroke risk not definitively proven
- Erythrocytosis caveat: May increase thrombotic risk
- Management: Aspirin if hematocrit elevated
Lipid Effects
Potential improvements: - Total cholesterol (within 6 months) - Triglycerides - Possible HDL decrease (not proven)
When to Discontinue
- No symptom improvement at 12 months
- Significant adverse effects
- Patient desire for fertility
- New contraindications (cancer diagnosis)
Tapering Considerations
- Avoid abrupt discontinuation
- Gradual dose reduction prevents symptom rebound
- Alternative: Transition to clomiphene if appropriate
XV. Clinical Pearls
-
"Treat the patient, not the number" - Symptoms matter more than absolute testosterone levels
-
Two-test rule - Always confirm low testosterone on separate days
-
Morning testing - Essential for accurate diagnosis
-
Sexual dysfunction focus - Primary evidence-based indication
-
12-month rule - Discontinue if no improvement
-
Cost considerations - IM injections significantly more cost-effective
-
Fertility discussion - Essential before treatment initiation
-
Specialist referral - When uncomfortable with management
XVI. Multiple Guideline Approach
Available Guidelines:
- American College of Physicians (ACP)
- Endocrine Society
- American Urological Association (AUA)
- UpToDate
Clinical Decision: Choose one institutional standard for consistency across practice.
Neurology
Neurology Inpatient
Neurology Inpatient
Attendings: Dr. Farooq and Dr. Showraki
Location
The neurology office is located at SGMC 5 South. There's a piece of paper taped on a door that says "neurology office" — it may be difficult to find at first.
Contacting the Attendings
- Dr. Farooq prefers you QliqCHAT her.
- Dr. Showraki you can text or call (217) 697-6760.
Both neurologists are friendly and will teach you — don't be afraid to ask questions. Dr. Showraki is more quiet/timid. The hours vary; usually you are done after didactics end.
Workflow
With Dr. Farooq
- Dr. Farooq will usually have you see two new consult patients in the morning.
- You will do a full H&P, present to her, and then write the notes.
- You will need to get her dot phrases, which you can find under her name on the Epic Smartphrases.
- Depending on the day, you will round on all her patients (follow-ups included) or just the new ones.
With Dr. Showraki
- Dr. Showraki prefers to write his own notes.
- You will only round on the most interesting patients with him.
- He will have you complete an NIH Stroke Scale course online. You'll receive a certificate you can put on your CV.
Code Strokes
If there is a code stroke, you will go to the ER and see the patient with whichever neurologist you are working with. Both neurologists will sometimes PIMP you, but it's really not that bad.
How to Prepare
Before starting, review:
- Hemorrhagic vs. ischemic strokes
- How to do a neuro exam
- NIH Stroke Scale
- Reading a brain MRI/CT
Tip
Don't forget your reflex hammer.
 Contributed by Brigita Eichler, MD
Contributed by Brigita Eichler, MD
Neurology Outpatient
Neurology Outpatient
Attending: Dr. Posas
Location
- Address: 4274 N Valdosta Rd, Valdosta GA 31602
- The building is near Smith Northview and has a large "SGMC Neurology" sign on it.
Hours
- Work hours begin at 8:00 AM.
- Clinic ends anywhere between 3:45 PM and 5:00 PM depending on the day.
- Tuesdays: Botox injections all day.
- Fridays: half days.
About Dr. Posas
- Child neurologist who did fellowship in neuromuscular disease.
- Very experienced (he's 69 and not planning to retire any time soon).
- Very nice and friendly, easy to talk with, and answers all your questions.
- Does not PIMP, and you don't write any notes.
Workflow
- In the beginning you shadow him.
- Later, he will send you to see patients by yourself and present them back to him.
How to Prepare
Before starting, read up on:
- Migraines
- Common nerve palsies
- Neuromuscular problems
- Anatomy of the muscles — important to know for Botox injections and EMGs.
Bonus points
He likes LSU and New Orleans a lot.
Contributed by Brigita Eichler, MD
Physical Medicine & Rehabilitation
PM&R Survival Guide
Physical Medicine & Rehabilitation Survival Guide
Daily Hours
You'll work Monday through Friday, starting at 7:00–7:20 AM. How late you stay depends on when patient care wraps up.
General Daily Workflow
- Show up at the Inpatient Rehabilitation Program (IRP) by 7:20 AM at the latest.
- Pre-chart and pre-round on patients.
- Dr. O's workflow is fluid — he may "run the list" and round with you during, before, or after you pre-round/pre-chart. He is very easy to get a hold of, so don't be shy to contact him if you need him.
- Head to the outpatient clinic for follow-ups, procedures, and NCV/EMG testing.
- Clinic usually wraps up around 5:00 PM.
- New admissions often come in after 5:00 PM, so expect to head back to the hospital fairly regularly.
Team Meetings
- Every Tuesday and Thursday at 12:15 PM. Plan on about an hour.
- You're excused from didactics these days, but team meetings are mandatory.
Outpatient Clinic
- Location: 3526 N Crossing Circle
- Use the side door. Code is 3526.
- The surgery center for procedures is adjacent. Some procedures are performed inside the outpatient clinic and some in the surgery center.
Computer Systems
Inpatient Login (Epic)
When you log in:
- Select "Direct supervision"
- Provider: Usman-Oyowe, Ibrahim
- Free type:
SGA IP REHAB PROV
Easy to miss
Change the service in the upper right corner of your note from Internal Medicine to Physical Medicine and Rehabilitation.
Outpatient Login (AthenaHealth)
You'll use AthenaHealth EHR. Your supervising physician will give you login credentials.
Documentation Tips
The "High-Risk Drug" Table
You'll see this on new patient and discharge notes. Fill it out based on what the patient is taking that day. Include daily prophylaxis anticoagulation if they're on it. For the diabetes/hypoglycemia risk line — if they have diabetes in any form, mark yes.
Daily Progress Notes
For the HPI, keep it brief — just hit the pertinent stuff. Use this template for the review of systems:
"Denies nausea, vomiting, fevers or chills. Denies any chest pain or shortness of breath."
Then edit it if the patient actually has any of those symptoms. Tack it on after your relevant HPI findings.
Time Documentation
Be sure the following statement exists on all daily notes:
"Time spent was 35 minutes with over 1/2 in direct patient care/examination, consultation with nursing, therapists, case manager and coordination of care. This progress note was dictated using voice recognition software. Please excuse any grammatical, word substitution or typographical errors."
Admission Notes
Common admission diagnoses you'll see: critical illness myopathy, debility, CVA.
Start your HPI like this:
"[Patient] was admitted to acute inpatient rehabilitation in the setting of [primary rehab diagnosis] status post [primary hospital problem]. Of note they have a prior history of [relevant past medical history]."
When you reconcile the Internal Medicine diagnosis list, keep as many as you reasonably can — they show complexity for billing. Internal Medicine keeps following these patients during their IPR stay, which means more eyes on them. Under each medicine diagnosis, you can write "Internal medicine on consult" after the basic management. You'll sit down with billing at some point to talk about covered vs. non-covered complicating diagnoses.
Discharge Notes
- Be sure to pend in the AM; prioritize doing these first.
- Discharge orders are typically put in the night before by Dr. O, and there will be a sheet of paper provided by the case manager specifying the logistics of the discharge. You will need this paper to complete the discharge note.
- If you're finishing the discharge note after the patient has already left, find them under "Recent Patients." Don't forget to add the attending's name back at the top.
- List any durable medical equipment (DME) recommended under the "Discharge Disposition" section, under a heading you type yourself stating "DME recommended".
Redundant heading
The discharge template has a redundant "Discharge Medications" heading near the end. Delete it — medications are already listed earlier automatically.
Functional History — The Important Part
This is probably the most critical piece of your discharge note. You're documenting how much assistance the patient needed on admission vs. discharge. This requires some detective work through therapy notes.
Assistance Scale
| Level | Meaning |
|---|---|
| 1 | Total assistance |
| 2 | Maximal assistance |
| 3 | Moderate assistance |
| 4 | Minimal assistance |
| 5 | Supervision / setup |
| 6 | Independent |
Where to Find the Info
- Mobility & Transfers: Check PT notes — "Plan of Care" section first, then "Notes".
- ADLs: OT notes — be specific about upper AND lower extremity needs.
- Cognition, Speech & Feeding: SLP notes (if applicable — not everyone gets speech therapy).
For admission status, use the initial evaluation from each discipline. For discharge status, you can use findings from up to three days before discharge.
Required
You MUST specify the level of assistance (min / mod / max assistance, etc.).
Daily Checklist
- [ ] 7:00–7:20 AM — Get to IRP, prep notes, pre-round
- [ ] Make sure service is set to "Physical Medicine and Rehabilitation" on all notes
- [ ] Finish daily progress notes with proper time documentation
- [ ] Head to outpatient clinic
- [ ] Tuesday/Thursday 12:15 PM — Team meeting (don't miss it)
- [ ] Watch for late admissions after 5:00 PM
- [ ] All admission notes due within 24 hours; daily notes by 4:00 PM
- [ ] Don't leave until your notes are done or unless excused by attending
Final Thoughts
- All discharge orders are performed by Dr. O.
- Admissions orders are typically done by him as well, unless otherwise specified. He will teach you how to put in admission orders if he expects that from you.
- It is also possible you may be released at 5 PM despite there being late admits. Take the schedule with a grain of salt; this may change if an NP is hired for full-time IPR.
Good luck on your PM&R rotation! Paying attention to documentation details keeps patients safe and billing accurate.
 Contributed by Sarah Sabol, MD
Contributed by Sarah Sabol, MD
Research Block
Research Block Intern Survival Guide
Research Block Intern Survival Guide
Overview
Before your research block begins, you'll receive comprehensive guidance from the program coordinator/director. This summary highlights key points from that resource, along with helpful tips to guide your preparation.
IRB Considerations
Important
The Internal Review Board (IRB) must be involved in virtually all research involving human subjects, including many secondary research projects.
- Consult with the Program Director early to determine whether your research requires IRB approval — this process can be time-intensive.
- Full IRB meetings occur only twice annually (July and January), so plan accordingly.
- Case studies may qualify for expedited review, and there's currently a proposal under consideration to streamline the IRB exemption process.
- Given these timelines, it's crucial to begin the IRB process well in advance of your planned research start date.
Mandatory Attendance
Daily Requirements
Safety Huddle — at least 8 sessions during your 4-week block.
- Time: 8:15 AM (Monday–Friday), lasts about 15 minutes.
- Location: Hallway behind the cafeteria. There is literally a HUGE white board that says Safety Huddle posted in the hallway.
Regular Meetings
- Didactic Sessions: Attend as usually scheduled. For any didactics you anticipate missing, you must get excusal from the PD — don't disappear.
- Mentor Meetings: Meet with the PD or your faculty mentor at least biweekly to assess progress.
Logging Hours
Don't forget to log "work from home" hours daily in New Innovations.
Required Assignments
1. CITI Training (MUST COMPLETE)
- Course: Medical Residents and Fellows: Basic Principles of Research
- Link: https://about.citiprogram.org/course/medical-residents-and-fellows-basic-principles-of-research/
Action items:
- Create an account.
- Meet with the Coordinator to pay for the course; the Coordinator will help you find the appropriate course in the list.
- Turn in the completed certificate by the end of the Research Elective via email to the program coordinator and director. You may or may not include your grade on the certificate — the option is given at the end of the course.
Pro tip
There are mini-exams at the end of each section. You can retake them as many times as you want, but your given grade at the end is calculated only on your first attempt.
2. Required Reading
QI Article: Mayo Clinic Proceedings QI article
- Also available on the public drive.
Final Deliverables
Due at the end of the elective.
Research Poster Presentation (slide format)
Format options:
- Research Posters: Introduction → Methods → Results → Discussion
- Clinical Vignettes: Introduction → Case Description → Discussion
Additional notes:
- Template available on the public drive (reach out to the Coordinator for access location).
- Optional: write an abstract for submission, but the poster slide is still required.
PowerPoint Presentation on a Research Topic
- Length: 10–20 minutes
- Audience: medical students and residents
- Topic: any aspect of research, QI, or patient safety
- Submission: email to the Coordinator and the Program Director.
Suggested Topics
Pick one (as outlined in the Research Document you'll receive at the start of the research block):
- Formulating a Research Question
- Study Design 101
- Introduction to Power and Sample Size
- Avoiding Bias in Clinical Research
- Basic Biostatistics for Residents / Med Students
- Common Statistical Mistakes in Resident Research
- P-values, Confidence Intervals, and Clinical Relevance
- How to Critically Appraise a Journal Article
- IRB Basics
- Translating Research into Practice: Residents in QI and EBM
- When does QI become Research?
Key Contacts
- Program Coordinator — for CITI payment and final submissions.
- Program Director / Program Mentor — for mentor meetings and final submissions.
Quick Checklist
- [ ] Attend 8+ Safety Huddles (8:15 AM, hallway behind the cafeteria)
- [ ] Attend all didactics as scheduled (get formal excusal if you need to miss)
- [ ] Schedule biweekly mentor meetings
- [ ] Complete CITI training and submit certificate
- [ ] Read required QI article
- [ ] Create poster presentation slides of the research you've been working on — consider creating an actual poster presentation
- [ ] Prepare a 10–20 minute PowerPoint presentation on a research topic
- [ ] Email final deliverables to Coordinator and Program Director
Tip
Consider typing out talking points under each slide of your PowerPoint. This isn't mandatory, but it looks cool and can help you if you have to present months later.
Contributed by Sarah Sabol, MD
Committees
List of Committees
Code and Rapid Response
Code and Rapid Response Committee
Code Team Training Committee Objectives
Curriculum Development
Develop a comprehensive curriculum covering:
- Code team roles
- ACLS protocols
- Documentation procedures
- Other relevant topics
Simulation and Training
- Conduct regular mock code simulations using high-fidelity mannequins
- Video record simulations for feedback and learning opportunities
- Include rapid response scenarios in simulation sessions
Process Improvement
- Streamline communication processes during code situations
- Establish a process to review all code events at the hospital
- Identify areas of strength
- Identify opportunities for improvement
- Analyze rapid response events similar to code analyses
Knowledge Enhancement
Ensure residents understand:
- Rapid response criteria and activation
- Supplies and equipment in code carts
Feedback and Continuous Improvement
- Provide structured feedback to residents involved in real codes
- Make recommendations to update processes/protocols as needed
Expert Involvement
- Bring in code team leadership to provide insights and expertise
Scenario Integration
- Practice transitioning from rapid response to code scenarios
Code & Rapid Response Committee Representatives
| Residency Year | Resident Name |
|---|---|
| First year | Shaleekha Sharma, MD; Margaret Jazayeri, MD |
| Second year | Moriamo Fashugba, MD |
| Third Year | Mariya Tom, MD |
Code and Rapid Response Resources
SGMC Code Blue Sheet
Code Blue Team: Roles & Responsibilities
Approach To Dyspnea
By Venkata Gandi MD, PGY-3 Mariya Tom MD, PGY-2 Moriamo Fashugba MD, PGY-1
Community Outreach and Fun
Community Outreach and Fun Committee
Community Outreach and Fun Committee Objectives
Community Engagement
- Identify and promote volunteer opportunities for residents in the local community.
- Organize health-focused community events (e.g., health fairs, free clinics, education sessions) in underserved areas.
- Encourage residents to apply their skills and knowledge for community benefit.
- Implement a system to track resident participation in community activities.
- Recognize and highlight outstanding community contributions by residents.
Social and Team-Building
- Plan and execute regular social gatherings for residents.
- Organize residency-wide events, including sports teams and group outings.
- Create opportunities for residents to socialize outside the hospital environment.
Wellness Initiatives
- Develop comprehensive wellness programs addressing common residency stressors, including burnout prevention.
- Establish and manage support groups for residents.
- Compile and distribute information on mental health resources available to residents.
Resource Management
- Identify and secure funding sources through grants, donations, and other means.
- Procure necessary supplies, equipment, and venues for committee events and initiatives.
Collaboration and Communication
- Maintain effective collaboration with other residency committees as needed.
- Develop and implement strategies for publicizing and promoting committee events and initiatives.
Community Outreach & Fun Committee Representatives
| Residency Year | Resident Names |
|---|---|
| First year | Julio Morciego, MD; Jan Perez Cajigas, MD; Jay Patel, MD |
| Second year | Ornob Rahman, MD; Michael Heron, MD; Rabail Shaikh, MD |
| Third year | Anna Ledford, MD; Mariya Tom, MD; James McSweeney, MD |
Community Outreach and Fun Resources
List of resources goes here
Diversity, Equity, Inclusion
Diversity, Equity and Inclusion Committee
Diversity, Equity and Inclusion Committee Objectives
Education and Awareness
- Develop a comprehensive curriculum on diversity, equity, and inclusion (DEI) topics
- Invite guest speakers and experts to share their perspectives on DEI issues
- Incorporate DEI principles into the residency curriculum and clinical rotations
- Provide resources to help residents develop cultural competency in patient care
Recruitment and Retention
- Ensure fair and unbiased recruitment practices for new residents
- Analyze demographic data to identify potential disparities in recruitment and retention
- Implement strategies to attract and retain a diverse pool of residents
- Provide support and resources for underrepresented minority residents
Inclusive Environment
- Foster an environment that values and respects different cultures and backgrounds
- Organize events and activities that celebrate diversity and promote cultural exchange
- Create safe spaces for residents to discuss DEI-related concerns
Support and Mentorship
- Establish a mentorship program that pairs residents with faculty from diverse backgrounds
- Offer counseling and support services for residents facing discrimination or bias
Continuous Improvement
- Regularly assess and improve DEI initiatives based on feedback and outcomes
- Stay informed about best practices in DEI and implement them in the residency program
Diversity, Equity and Inclusion Committee Representatives
| Residency Year | Resident Name |
|---|---|
| Second year | Asma Yasin, MD |
| Third Year | Hala Sharma, MD |
Diversity, Equity and Inclusion Resources
List of resources goes here
Education & Research
Education and Research Committee
Education and Research Committee Objectives
Curriculum Development and Management
- Develop a comprehensive educational curriculum aligned with program goals and accreditation standards
- Ensure curriculum covers core competencies, procedural skills, and various medical specialties
- Incorporate evidence-based teaching methodologies and innovative learning strategies
- Regularly review and update the curriculum to reflect the latest medical advancements
Educational Sessions
- Organize regular resident conferences, grand rounds, and didactic sessions
- Invite guest speakers and experts to share their knowledge and experiences
- Encourage resident participation through case presentations, journal clubs, and research updates
Mentorship Program
- Establish a robust mentorship program to support residents' academic and professional development
- Pair residents with faculty mentors based on their interests and career goals
- Provide guidance on research project selection, study design, and manuscript preparation
- Offer career counseling and advice on fellowships, job opportunities, and academic pathways
Research Support
- Identify potential research areas and encourage residents to pursue scholarly projects
- Assist residents in obtaining funding, navigating IRB processes, and securing resources
- Provide training on research methodology, data analysis, and scientific writing
- Facilitate opportunities for residents to present their research at local, regional, and national conferences
Assessment and Evaluation
- Implement a comprehensive assessment program to monitor resident progress and competency attainment
- Utilize various assessment tools, such as objective structured clinical examinations (OSCEs), simulation scenarios, and in-training examinations
- Collect and analyze data to identify areas for program improvement and curricular enhancements
Collaboration and Networking
- Foster collaborations with other departments, institutions, and research organizations
- Encourage residents to participate in interdisciplinary research projects and multi-center studies
- Facilitate networking opportunities with academic leaders, researchers, and potential employers
Committee Management
- Work with chief residents under the guidance of academic attendings to execute all committee objectives
Education & Research Committee Representatives
| Residency Year | Resident Name |
|---|---|
| First year | Mafaz Mansoor, MD; Rawa Salih, MD |
| Second year | Rabail Shaikh, MD; Patrick Joseph, MD |
| Third Year | Hala Sharma, MD |
Education and Research Resources
List of resources goes here
EKG
EKG Committee
EKG Committee Objectives
Curriculum Development
- Create a structured EKG curriculum covering basic to advanced concepts
- Outline learning objectives and competencies for each training level
- Stratify cases based on difficulty for residents at different training levels
- Develop modules on systematic EKG interpretation, rhythm analysis, bundle branch blocks, etc.
Interactive Learning
- Incorporate interactive cases, self-assessments, and knowledge checks into the curriculum
- Organize regular EKG reading sessions with faculty experts
- Utilize audience response systems or apps for interactive learning
- Conduct EKG competitions or games to enhance engagement
Resource Development
- Curate a comprehensive online database of annotated EKG cases
- Include examples of common and rare EKG findings in the database
- Provide access to reference materials, guidelines, and up-to-date resources
Innovative Teaching Methods
- Explore virtual reality or 3D simulations for spatial EKG understanding
- Arrange sessions practicing EKG acquisition on simulated patients
Clinical Integration
- Integrate EKG skills into procedures, codes, and clinical rotations
Continuous Improvement
- Regularly review and update the EKG curriculum based on feedback and new developments
- Assess resident progress in EKG interpretation skills and adjust teaching methods as needed
EKG Committee Representatives
| Residency Year | Resident Name |
|---|---|
| First year | Rawa Salih, MD; Genesis Munoz, MD |
| Second year | Ornob Rahman, MD |
| Third Year | Brandon Rockwell, MD |
EKG Resources
List of resources
Jeopardy
Jeopardy Committee
Jeopardy Committee Objectives
Question Development
- Create a systematic process for developing Jeopardy-style questions and answer banks
- Establish categories covering various medical topics, specialties, and levels of difficulty
- Involve residents in writing and vetting questions to ensure quality and relevance
- Explore the use of multimedia elements like images, ECGs, or radiographs in questions
Event Planning and Coordination
- Plan and coordinate regular Jeopardy competitions or tournaments
- Determine formats (team-based, individual, etc.) and rules for the competitions
- Secure venues, equipment (buzzers, scoreboards), and any necessary resources
- Promote the events effectively to maximize resident participation
Resident Involvement
- Encourage residents to take leadership roles in organizing and hosting the competitions
- Provide opportunities for residents to moderate and manage the Jeopardy games
Educational Impact
- Provide feedback on the rationale and explanations for correct and incorrect answers
- Identify knowledge gaps and areas for improvement based on competition performance
Motivation and Recognition
- Explore creative incentives like CME credits, gifts, or special privileges
- Recognize and celebrate the achievements of participants and organizers
Team Building
- Foster a spirit of friendly competition and camaraderie among residents
- Use the Jeopardy events as opportunities for socializing and team building
Continuous Improvement
- Regularly review and update the question bank to ensure relevance and accuracy
- Collect feedback from participants to enhance future events
Jeopardy Committee Representatives
| Residency Year | Resident Name |
|---|---|
| First year | Mafaz Mansoor, MD |
| Second year | Sandhya Lakkireddy, MD |
| Third Year | Taylor Martin, MD |
Jeopardy Resources
List of resources
POCUS
POCUS Committee
POCUS Committee Objectives
Curriculum Development
- Establish a comprehensive POCUS curriculum spanning introductory to advanced levels
- Define clear learning objectives and competencies for each training stage
- Develop modules covering ultrasound physics and image optimization
- Include modules on specific POCUS applications (FAST, cardiac, lung, vascular, etc.)
Hands-on Training
- Coordinate regular hands-on scanning sessions on simulation models and volunteers
- Ensure adequate access to ultrasound machines for resident practice
- Integrate POCUS training into relevant clinical rotations and procedures
- Explore opportunities for one-on-one preceptorship with POCUS experts
Image Review and Interpretation
- Organize regular image review sessions focusing on image acquisition and interpretation
- Utilize a cloud-based platform for sharing, annotating, and discussing POCUS images
- Encourage residents to log and track their POCUS scans for feedback
Simulation and Assessment
- Incorporate POCUS into simulation scenarios for integrated training
- Develop objective structured clinical examination (OSCE) stations for POCUS assessment
- Provide structured feedback on POCUS skills during clinical rotations
Credentialing and Certification
- Identify appropriate POCUS credentialing pathways for residents
- Assist residents in obtaining POCUS certifications recognized by professional societies
Compliance and Policy
- Ensure compliance with institutional policies and billing requirements
Continuous Improvement
- Regularly review and update the POCUS curriculum based on technological advancements and clinical practices
- Collect and analyze resident feedback to enhance the POCUS training program
POCUS Committee Representatives
| Residency Year | Resident Name |
|---|---|
| First year | Rawa Salih, MD; Issac Brian, MD; Paul Reese, MD; Brigita Eichler, MD; Karam Randhawa, MD |
| Second year | Samuel Edusa, MD |
| Third Year | Justin Owens, MD |
POCUS Modules
1. Introduction to POCUS
An introductory course on Point-of-Care Ultrasound (POCUS) covering probe types, imaging units, and techniques for obtaining interpretable images. Learn machine operation basics, hands-on probe placement and manipulation skills, and image interpretation fundamentals.
NOTE: Please complete the module and email your certificate of completion prior to the hands on session.
2. Cardiac POCUS
An interactive course on cardiac ultrasound imaging fundamentals. Learn to obtain five standard cardiac views, evaluate the inferior vena cava, and identify pericardial effusions and other pathologies, enhancing your diagnostic skills. Prerequisite: Introduction to POCUS
NOTE: Please complete the module and email your certificate of completion prior to the hands on session.
3. Central line and A lines
4. Lung POCUS
Explore advanced POCUS techniques for lung and chest assessment. This interactive guide covers standard image acquisition, recognition of normal lung ultrasound artifacts, and identification of pneumothorax and other pathologies. Prerequisite: Introduction to POCUS
NOTE: Please complete the module and email your certificate of completion prior to the hands on session.
5. Abdominal POCUS
Intra-Abdominal Free Fluid
An interactive course introducing the essential skills for detecting and visualizing free abdominal fluid with ultrasound. Learn to acquire images confirming the presence or absence of significant intra-abdominal free fluid. The course also covers common pitfalls and limitations in evaluating intra-abdominal free fluid. Prerequisite: Introduction to POCUS
NOTE: Please complete the module and email your certificate of completion prior to the hands on session.
Urinary System
An interactive course preparing you for hands-on POCUS training to detect and visualize the urinary system. Learn four indications for urinary system POCUS, review normal and pathological kidney scans, and acquire practical tools including bladder volume measurement and a systematic process for integrating urinary POCUS into clinical evaluation. Prerequisite: Introduction to POCUS
NOTE: Please complete the module and email your certificate of completion prior to the hands on session.
Women In Medicine
Women in Medicine Committee
Women in Medicine Committee Objectives
Mentorship Program
- Establish a robust mentorship program pairing residents with female physician mentors
- Facilitate networking opportunities between mentors and mentees
- Provide mentorship training for effective guidance and sponsorship
Professional Development
- Organize workshops on negotiation skills, leadership training, and career planning
- Bring in female physician leaders across specialties to share their journeys
- Discuss topics like implicit bias, workplace discrimination, and work-life integration
Wellness Initiatives
- Plan wellness activities tailored to common concerns for women in medicine
- Address issues like maternal health, work-family balance, and burnout
- Provide resources for mental health, counseling, and support groups
Awareness and Education
- Develop educational materials on gender-specific challenges in medicine
- Organize events to raise awareness about women's contributions to medicine
Advocacy
- Identify and address systemic barriers for women in medical education and practice
- Collaborate with institutional leadership to promote gender equity policies
Networking and Community Building
- Create opportunities for women residents to connect and build supportive relationships
- Organize social events and informal gatherings to foster a sense of community
Research and Data Collection
- Encourage and support research on women's experiences in medicine
- Collect and analyze data on gender disparities within the residency program
Continuous Improvement
- Regularly assess the effectiveness of committee initiatives and adapt as needed
- Seek feedback from residents and mentors to enhance program offerings
Women In Medicine Committee Representatives
| Residency Year | Resident Name |
|---|---|
| First year | Zoha Allahuddin, MD; Srujitha Ravuri, MD |
| Second year | Rabail Shaikh, MD |
| Third Year | AmandaNell Shook-Chacon, MD |
Program Directory
Protected page
Enter the password to view the directory and save people to your contacts.
Best to be saved on a mobile device.