Guide to Medicine Wards
Who to ask for help/clarification?
- Your supervising resident
- Chief Residents: Samuel Edusa, MD and Ornob Rahman, MD
- Attendings: Dr. Lamptey, Dr. Gallagher, Dr. Sobukonla, Dr. Matthew Varn, Dr. Roberta Baah-Sackey, Dwayne Mohan, MD, Rosaida Silverio-Lopez, MD, and Venkata Gandi, MD
- For outpatient questions: Dr. Bias
- Administrative questions: Ms. Dawn Marro and Ms. Tonya Moreno
Helpful Resources
- Open Evidence: AI-powered platform that aggregates and synthesizes peer-reviewed medical literature to help healthcare professionals make evidence-based decisions at the point of care through research summaries, article links, and current clinical guideline.
- UpToDate: Clinical decision support tool that provides evidence-based medical information and treatment recommendations to healthcare professionals at the point of care.
- University of Chicago House staff Guide (for critical care, heme/onc, procedures).
- Life in the Fast Lane (LITFL): Medical education website providing emergency medicine and critical care resources including clinical cases, ECG interpretation, medical mnemonics, and point-of-care learning materials for healthcare professionals
- Timeofcare.com: Website with common work-up orders for inpatient and outpatient medical conditions
- Sanford guide: Comprehensive antimicrobial therapy reference that provides healthcare professionals with evidence-based recommendations for antibiotic selection, dosing, and treatment duration for infectious diseases.
- MDCalc: Medical calculator platform that provides healthcare professionals with validated clinical decision tools, risk scores, and diagnostic calculators to support evidence-based patient care decisions.
- MKSAP: American College of Physicians' continuing medical education program that provides internal medicine questions, case studies, and educational content for board preparation and ongoing physician learning.
EPIC tips/adjustments
Prior to starting your inpatient rotation:
- Adjust your Epic print settings
- Add your favorite orders
- If not already available, create a
My Listsection to add your assigned patients. - Always right click on the patient's name and
Assign mewhen given a patient to work with. - Also send it to your list by clicking
Send toand thenMy list. - You should also add the patient to the
Night Medicine Residency list.
Example of how to setup your Epic Tabs
Include on your printed handoff the following items by right clicking on your My list, clicking Properties, and below at Selected columns, have the following:
- Room/Bed
- Patient Name
- Age/Gender
- Blank column
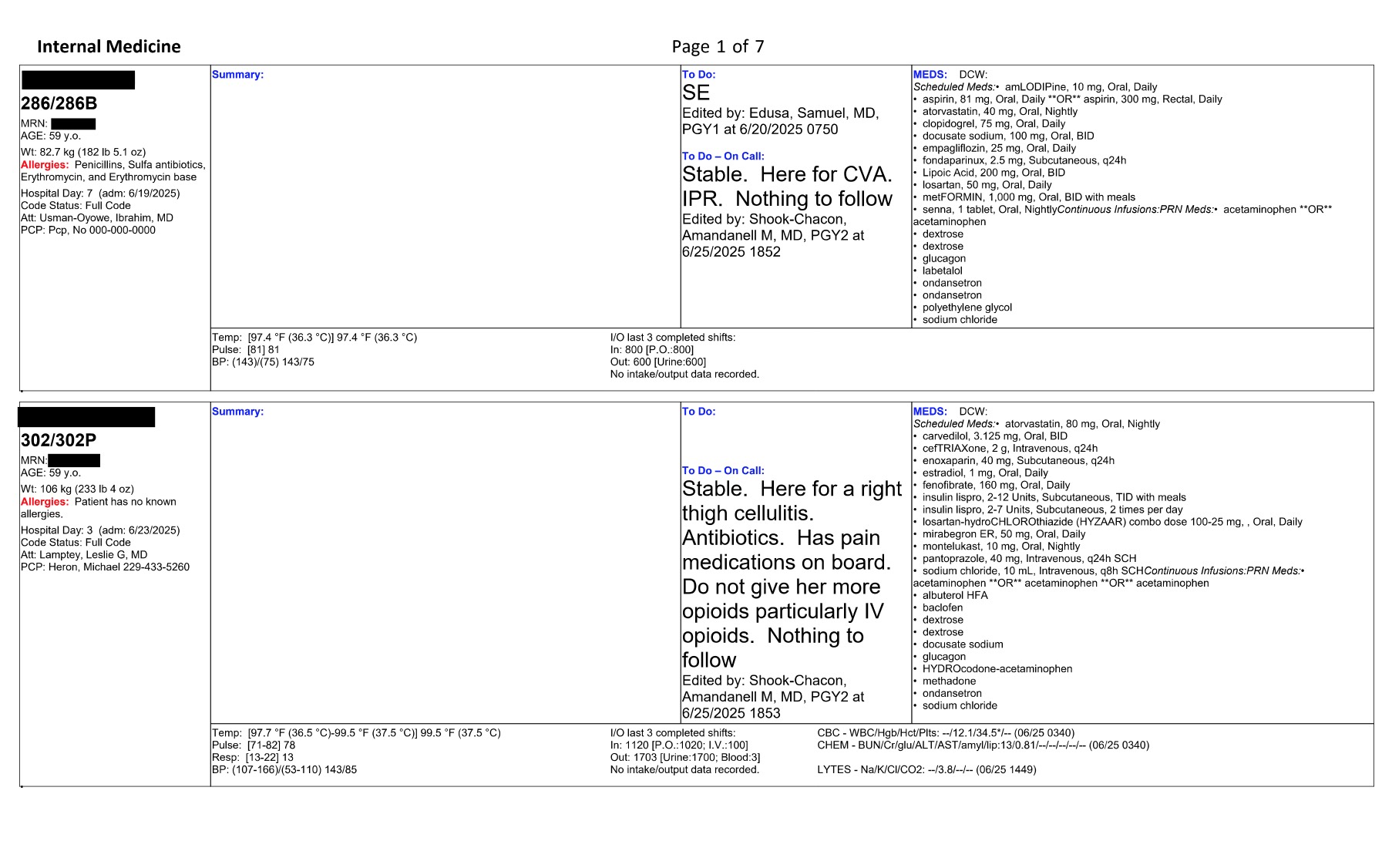
This should print the following:
- Patient's name and room number
- MRN, age, weight, allergies, admission days, date of admission, code status, attending, PCP
- Empty summary box
- Last recorded vital signs with lowest and highest value in the last 24 hours including temperature, pulse, respirations, blood pressure, and FiO2%
- I/O for the last 3 completed shifts, quick overview of CBC (it won't include WBC), chemistry, electrolytes (it won't include glucose) and medications
Example of a handoff
To add to your favorite orders:
-
Go to
Ordersand on the right-hand search box, there is aNewbutton, click on it and it will allow you to search for physicians' favorites. i.e. If you search forAgrawalinSearch order sets and panels by user, you will findadmission orders, anddischarge ordertemplates. You can add them to your favorites and select or unselect as you work with your admissions. -
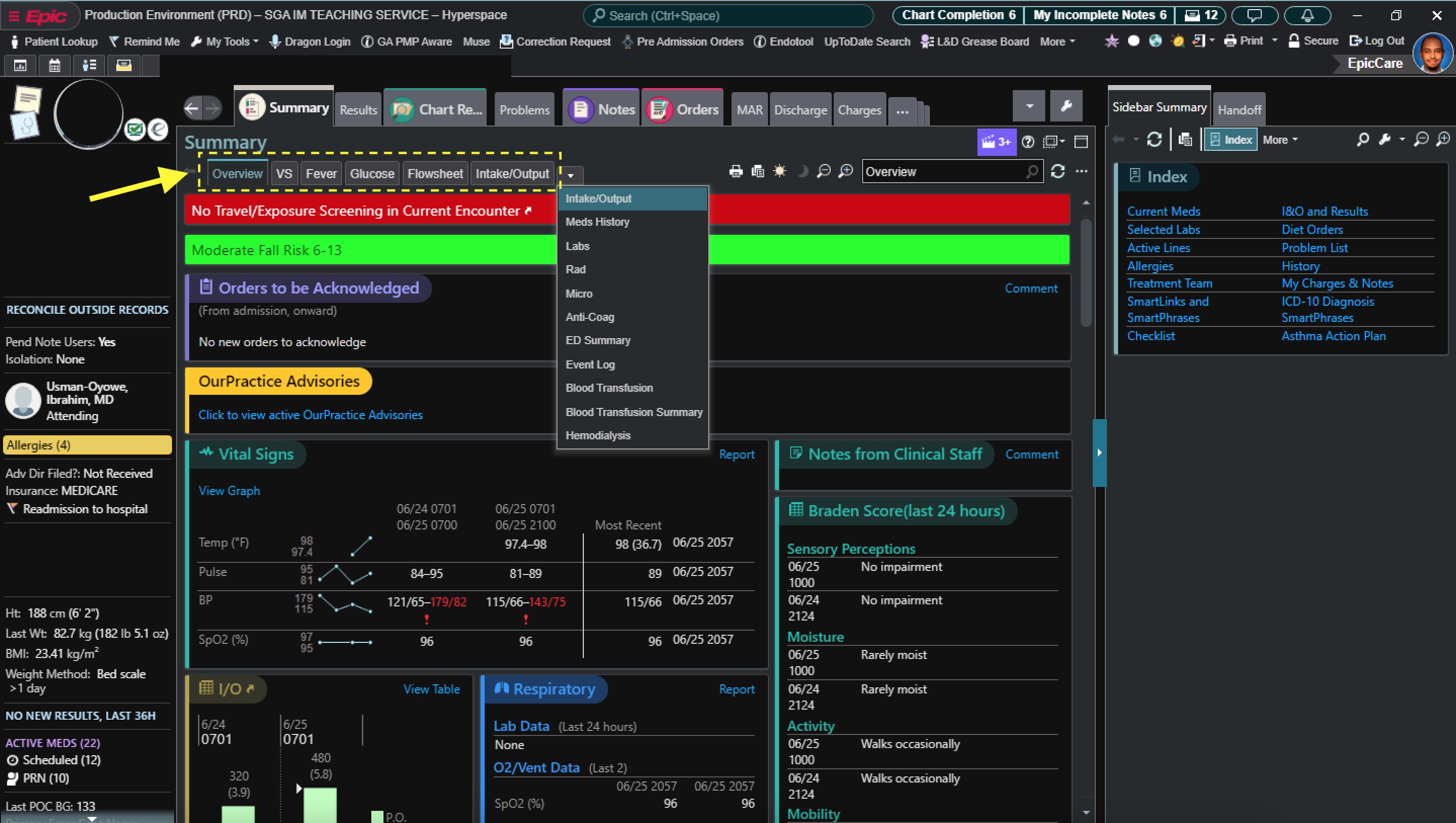
For a full report of laboratory results, in the summary section, add
Labs. This will simplify your view of completed labs to date in the present admission.
Getting into action...
To have a successful rotation, it is recommended that you:
- Apply good teamwork
- Proper communication
- Call your consults early
- Stay proactive, and remain available to your patient and team's needs.
Other Important Tips
- Be nice to everyone (nurses, RTs, consultants, ED team, peers). Professionalism is key.
- Follow your chain of communication.
- Set expectations upfront with your senior resident/attending (i.e. how often should interns check in with seniors, etc.).
- Always ask your senior resident if you are unsure of something.
- Important things to inform your senior resident include changes in vitals (fever, tachycardia, hypotension/hypertension), hypoxemia or increasing O2 requirements, new altered mental status, significant lab abnormalities, or other significant change in patient status.
- Return calls or secure chat messages in a timely manner (<10 min). Triaging pages in order of importance is vital to good patient care.
- Update the nurses after rounds with the plan of care for the day.
- When entering NPO order, write the reason for NPO in the comments section.
- When pt is NPO, make sure to adjust insulin as needed (see DM section). Talk to your senior for help.
- If pt is NPO for several days, consider maintenance IF fluids (MVIF) (eg, D5NS at 75 ml/hr) vs enteral nutrition via NGT.
- If pt is NPO overnight for an AM test/procedure, no need to give MIVF.
- When ordering IV antibiotics, always think about age, kidney function, and indication. If you're unclear on a dose - call pharmacy, they will help you. Also check previous
Microsection for past positive cultures and susceptibility.
Before you start wards:
- Meet with your teammates and review your inpatient schedule. Your schedule will be provided prior to the start of your rotation. Chief residents arrange long call vs short call days along with days off.
- Ensure your teammates have your contact number. Remember to use Qliq when messaging about patients.
- Message your supervising resident. Let him/her know you are excited to start working in this rotation with them and inform them of your clinic days. They may message you and your co-intern together in a common group text. They may or may not include the attending as well.
- Also remember, you are a team. If one intern is running a little late, help your co-intern and reach out. If you move somewhere in rounds, communicate, and let your co-intern/resident know where you are.
- If you must give information to the resident or attending about your co-intern's patient, give your co-intern a head up beforehand when possible.
- Review the calendar days for noon report and mark them early so you can start thinking of interesting cases to present and can prepare with enough time.
- Get sign out from the current inpatient team and know what patients you will be taking over. This usually happens the day prior to starting your rotation. Your patients are assigned by your supervising resident or attending.
Layout of a full day in wards (This layout may vary depending on team or rotation changes, please be flexible and open to)
Preparing for rounds
-
(1) Arrive between 5:30 – 5:45 AM. You might need to adjust your arrival time prior to or after getting used to the system and flow of work.
-
(2) 5:30-6:30 AM. Pre-chart. Pre-charting is the practice of reviewing the patient's record to get a better understanding of the patient's overall health status and the plan of care.
Tip
When pre-charting, here is a summary of the sections that you can access in EPIC:
- Chart Review: To see previous notes, labs, images…
- Summary: Labs, radiology, micro, cardiology (to see EKG), reconcile (to see what meds they had at home).
If you notice labs that need to be ordered or tests that should be done early or pertinent/urgent abnormalities that need to be addressed suggest before rounds.
Read the ED notes to get an idea of what's going on with the patient. If the patient has already been admitted, review H&P and consult notes.
Dr. Brown, ID attending, in his ID expectations provides an excellent detailed layout on how to thoroughly review a chart. You can access it in the Internal Medicine Residency General Guide.
-
(3) 6:30-7:00 AM Go talk to night nurses before shift change at 7:00 AM. Check in with them and verify if anything happened overnight.
-
(4) 7:00 AM Get sign-out in the GME area. This might be slightly delayed depending on the night team. If you're signed out a patient as being sick - see them/check vitals/labs FIRST. You can message your senior urgently if you see them and the patient has concerning findings.
-
(5) 7:15-8:15 Go see the old and new patients. Return to the GME area and start writing notes. In the subjective portion of the notes, include overnight events, patient's overall status, complaints.
-
(6) Be ready for rounds by 8:30-9:00 AM. Attendings will usually come to GME. Some attendings would want to see you directly in 3W/4W/Tower. Clarify with your senior the location where rounds will start and be on time.
-For some attendings rounds will start by seeing patients that are potential discharges first. Some attendings would want to see very sick patients first. Try not to discharge or transfer before rounds unless the attending tells you to do so. - Anticipated discharges still need an order for discharge on the day of discharge. - If you are asked to transfer a patient, under
Ordersplace a new order by typing Transfer patient. Then select where you would want to transfer the patient. To finalize, go to theTransfertab and decide what orders will continue upon transfer. - Anticipated discharges still need an order for discharge on the day of discharge.
During rounds
- Present patients.
Note
Example of presentations
- Attending A: PMH, CC, HPI, physical exam, pertinent labs, imaging, assessment, and plan per problem.
- Attending B: Why is the patient here? What are we doing for the patient? Why can't the patient go home today?
- Attending C: Subjective (PMH, CC, HPI), Objective (vitals, labs, images, physical exam), Assessment and plan.
-
Get orders to put in and confirm assessment and plan if necessary. Have pen and paper to write down plan. If unclear, verify with resident/attending. Some orders are critical and may require immediate attention. If so, place them via Haiku on your phone, but know that some consults and orders cannot be placed via Haiku. If unable to use Haiku, try to find a computer station close by, and enter them quickly.
-
Rounds end around 11:30 AM-12:00 PM. If participating in half-days at the clinic, make sure your resident/attending knows where you stand with note status and patient care. Before leaving for the clinic, do a brief sign-out to the resident and inform labs/results to follow-up on.
-
After rounds, at 12:15, be ready for noon report/lectures. If you are presenting, let your supervising resident and team know. You will pick a patient for the report days prior to prepare well. This case should be preferably a new admission that you learned a lot from or a patient with an interesting diagnosis. It could also be a “bread-and-butter” case, and if possible, provide a good teaching point at the end of your presentation.
After rounds/noon report:
- Place orders
- Write notes
- Some attendings will review the plan of care and perform a second round.
- You may need to check on sick patients again.
End of the day:
- All notes finished.
- Relevant events that occurred during the day and must be informed right away include pertinent notifications from nurses, changes in vitals, pertinent labs that needed replacements, important orders that were put in, new imaging findings or updates from consultants.
- Review consult recommendations especially if patient is surgical. If surgery is anticipated in the AM, make sure NPO orders are in starting midnight. If needed, hold anticoagulation/DVT prophylaxis, and make sure PT/INR, aPTT, type and screen is ordered if applicable. If patients receive night insulin and they are to be NPO, consider decreasing dose or holding for that evening to avoid hypoglycemic events.
- Call family and update on plan of care.
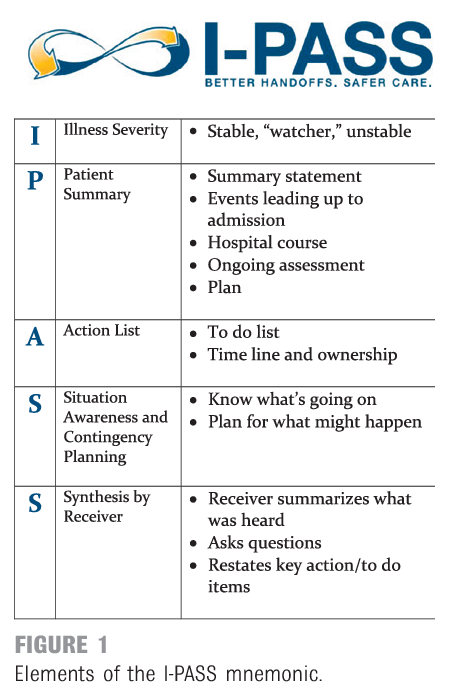
- Get ready to sign-out with the cross-coverage team. Update the Night Medicine residency list. Use IPASS (see figure below) for your sign-out.
If you are short call, you may leave at 3:00 PM if all your work is done and you have been cleared to go by your senior. Prior to leaving, you are responsible for signing out to the cross-coverage team. Remember to forward any Qliq messages and notifications to the cross-coverage team or the night team if received after 7:00 PM.
If you are long call, you are responsible for printing the list for all teams for start of the day census. You will put in the administrative office by GME, along with the admission sheet from the night before. You will be responsible for receiving all the admission calls and receive floor calls for all teams. You should also have available an admission sheet documenting the admissions your team receives during the day. You will be responsible for both call phones. (229-561-4596/229-5614597). You will stay to provide sign-out to the night team. Your admission time ends at 6:15 PM. If you receive an admission after, you might save it for the night team. Still, obtain a full report from the ED so you can provide the admission details to the night team.
See below an acronym you may use during sign-out. Also remember to highlight CODE STATUS.
Layout of a full day in wards, in summary
- Pre-chart.
- Get sign-out on patients from covering night team at 7:00 AM. You may get signed out overnight admissions depending on where you are in the call cycle.
- See all patients (unless pre-determined with your team).
- Replete electrolytes, order blood prn.
- Start (ideally finish!) progress notes.
- Be ready for rounds from 8:30-9:00 am to 12 pm.
- Afternoons are typically for catching up on tasks, finishing notes.
- Sign-out to the cross-cover or night float team when your senior tells you it's okay.
- Contact family and update on plan.
- Night float typically begins cross-cover at 7pm – confirm with your senior.
Tips/Common Questions
- If a patient is admitted for hypoxia, know the O2 Sat, if they have blood gases, what are their values? How would you interpret them? How much oxygen is he on?
- When typing a note, it's better to be precise with important information.
- Hypocalcemia? Always look for albumin and correct.
- Hyponatremia? Correct if diabetic and hyperglycemia is present.
- DKA when is it resolved? When the anion gap closes.
- Patient with SVT and stable first thing to do: Vagal maneuvers.
- On the days you have clinic, you might need to be more proactive.
- Avoiding arrhythmias is worth it. Use the "2–3–4–9" rule to remember the desired levels of magnesium, phosphorous, potassium, and calcium, respectively.
-
Know the seven Ps for each of your patients: Problems, Progress, Pain, PO (oral intake), Pee-Pee, Poop, and Physical condition.
Problems: refers to the problem list you are addressing for the patient (i.e., why and how the patient came to be under your care) and what you are doing for each with respect to either diagnosis or treatment.Progress: refers to the events in the past twenty-four hours that have happened positively or negatively to your patient. Progress is what the team will want to hear about every day.Pain: Assess your patient's pain and adjust medications so the patient is reasonably comfortable.PO: Know how your patient is getting nutrition and how far you can advance his or her diet. Patients should be NPO (taking nothing by mouth) post-surgery until they have bowel sounds; then clear liquids may be started, and continued until the patients pass flatus, when solids may be tried. Do not be afraid to go slowly or take a step back. If a patient is not taking food by mouth, note the nutritional route or the reason for withholding oral nutrition; if he or she is eating, know the type of diet (e.g., clear liquid, dysphagia ground, diabetic, low salt, regular). Know your patients' urine output and if it is adequate (i.e., at least 30 mL/hour; perhaps less for children and the elderly) and the route (i.e., via catheter or naturally).Pee: If a patient is off a patient-controlled analgesic (PCA) or other, more-invasive pain control (e.g., an epidural catheter) as well as able to sit on a bedpan or use a urinal, get that foley catheter out. When removing a foley catheter, be sure to write for bladder scan after six hours if the patient has not urinated, and to replace the Foley catheter if the bladder scan is more than 350 mL.Poop: Assess the number of days since the patient's last bowel movement so you know how to adjust bowel care.Physical condition: Understand the patient's physical condition and progress with physical, occupational, and speech therapy as well as all other consults required to aid in the management of the patient's case.
Admissions
- You will get a call from the ER doctor. While on the call take notes on name, location, PMH, CC, what has been done for the patient, orders they want you to follow up on, and why the patient is being admitted. If possible, do a quick review of the chart while on the call and ask questions.
- Once you have the patient localized on Epic, assign yourself to the patient by right clicking on the patient and selecting
Assign me. Double click on the patient and open the chart. Go to the Summary tab. In the Comment section, enter the dot phrase.RESPTto include the call phone contact disclaimer. Send the patient to your team’s list and the night medicine list. - Inform your resident. Ask if you should admit right away or go see the patient, evaluate, and then if appropriate put a general admission order to either Inpatient or Observation. This will likely depend on severity. Ask the resident where to admit the patient to. In most cases, you will admit to inpatient if care/hospital stay is predicted for at least 2 midnights. If this patient is expected to stay less than 2 midnights (diagnostic examples: TIA, CVA rule out, syncope, other), you may place in observation status. Talk with your supervising resident and put overall admission orders together.
- When you go see the patient, get HPI, thorough medical history and physical exam, think of assessment and plan, think of additional orders. If family is present, make sure to obtain contact number and add information to chart if not available before. Address CODE STATUS for all your admissions. Discuss the patient with your resident. Work on your H&P note, and then be ready to discuss and present to your attending.
- The flow of admissions may vary depending on teams and attendings.
Admission Checklist
- Assign yourself to the patient and add to your patient list and night medicine list.
- Look at admitting diagnosis and vitals.
-
Chart review:
- Look at ED notes and interventions (you can find ED clinical summary under summary tab which tells you when they got fluids etc.)
- Look at previous discharge summaries
- Look at results (labs/imaging)
-
Place basic orders. Observation status vs inpatient.
-
Go and see pt and obtain HPI
- If a patient looks acutely ill, call senior.
- Obtain HPI, PMHx, etc. Do physical exam.
- Reconcile med list / Order appropriate home meds – this includes calling patient's pharmacy and confirming meds are correct- if theirs is closed, see if there is a 24hr one available
- Confirm code status (place order)
-
Staff the patient / discuss with senior
-
Place admission orders. (Usually General Adult Admission order set, but look! There are often disease-specific order sets available).
- Hold diet until talk to pt and you are sure that no interventions that might require NPO
- Order DVT ppx – make sure plts >50k on labs and no other contraindications, also choose correct ppx for CrCl (<30 heparin, otherwise Lovenox— which is much better since it’s once daily vs. two- three times daily. and requires no surgical interventions). You may use Xarelto if patient is stable, tolerating PO and with no potential surgical dx.
IMPORTANT: All admission orders should include the following PRN meds:
- Tylenol 325-650mg q4h prn for mild pain or headache (2g max in cirrhosis). You can put in comments to "call for fever." Unless liver disease, high LFTs.
- PRN for constipation (i.e. Miralax 1 packet once daily prn (or a bowel regimen of your choosing)).
-
Sign and hold orders if still in ED.
-
Final Orders
- Make sure home meds are correct
- Place any additional orders discussed in staffing
- Confirm that orders match the written plan
-
Finish writing H&P
Progress Notes
- Subjective: a quick outline of important events in the last 24 hours, issues the nursing staff has mentioned that the patient may not have, any updates on their condition that the patient mentions to you (worsening nausea, improved pain)
- Vitals: they are vital and must include numbers in a range of lows and highs over the last 24 hours; afebrile is not a vital sign.
- I/O’s: include totals in and out as well as specifics (what amount out was urine, how much was stool, how much was vomitus)
- Meds: copied into the note and updated daily. This is a great time to make sure medications are renewed and adjusted appropriately
- Physical Exam: system based, highlighting pertinent data/findings on examination. You may include media pictures for skin findings.
- Labs/Imaging/EKG: include daily labs, pending or completed culture results including sensitivities, any new radiographic studies, EKG if applicable performed since the last note you wrote.
- Before your Assessment/Plan you may include a quick, one-liner including the patient’s age, sex and primary problems for current presentation.
- Assessment: Describes the diagnoses, attributable cause and your subjective/objective data to support the diagnosis.
-
Plan: List this out by the issues
- Each problem should be listed separately along with what you plan to do about it that day and what was done about it the day before
- Any problem which has resolved in the last 24 hours should be listed one last time to acknowledge its resolution and then can be dropped from the list If you don’t know the specific plan on an issue, you may write, to be further discussed with team – an addendum note can always be completed later
-
Be sure to mention prophylaxis daily (Nexium, SQ heparin, SCD’s) in every note
- Always end your note with CODE status
- Document family discussions
Discharges
- Daily discussions with your seniors/attendings and social worker/case manager/nurses/families are crucial for a proper discharge process. It is imperative that you update social workers on each floor on discharge planning. Review PT/OT notes for placement recommendations and provide prompt instructions to social workers/nurses along with family members. Placement at rehabilitation facilities varies depending on physical needs and are sometimes subject to insurance approval.
- Placement considerations:
- (1) SNF: Skilled nursing facility. Examples of patient needs: Prolonged IV antibiotic course, ongoing 24-hour nursing care, patients that live in SNF already, unable to care for self if living alone. This provides a more medical-like environment than assisted living facilities.
- (2) SB: Swing-bed. Examples of patient needs: Need for rehabilitation in hospital-like facility, need for strength recovery prior to discharge home, post-surgical patients.
- (3) Assisted living facility: Examples of patient needs: Patients are independent with good ADLs tolerance but live in a facility with household similar accommodations.
- (4) IPR: Inpatient rehabilitation facility. Examples of patient needs: Patients with more intense rehabilitation needs, that are able to participate actively in therapy. At times, they have medical conditions that require monitoring/optimization. This is in-hospital rehabilitation.
- (5) Home with home health +/- PT/OT. Examples of patient needs: Patients that will require visits for at home assistance with monitoring of medical conditions or PT/OT. They typically require less intense rehabilitation measures.
- (6) Hospice: At home or facility. Recommended after a Palliative Care consult.
Discharge Checklist
- Go to
discharge navigator. -
Must do on each patient:
- Med Rec: THIS IS ONE OF THE MOST IMPORTANT THINGS WE DO so it should be done correctly. Ask your senior to help you or check it once you are done
- Follow up Providers: It is better to schedule follow-ups then rely on your patient to do so
- PCP communication: Underrated but so important. Ideally PCP should be called every hospital stay.
- Pt hospital summary: Use this instead of D/C instructions because it'll go on the top of the AVS instead of bottom. You can put stuff in D/C instructions over the course of their stay as it is a working document of sorts (unlike the pt summ) and then just copy and paste into pt summary on day of discharge
- D/C Summary: Remember busy PCPs are reading these so keep it as concise as possible. Be sure to document changes in meds, pending labs, things you want them to do.
- Preview AVS then sign AVS/CoC
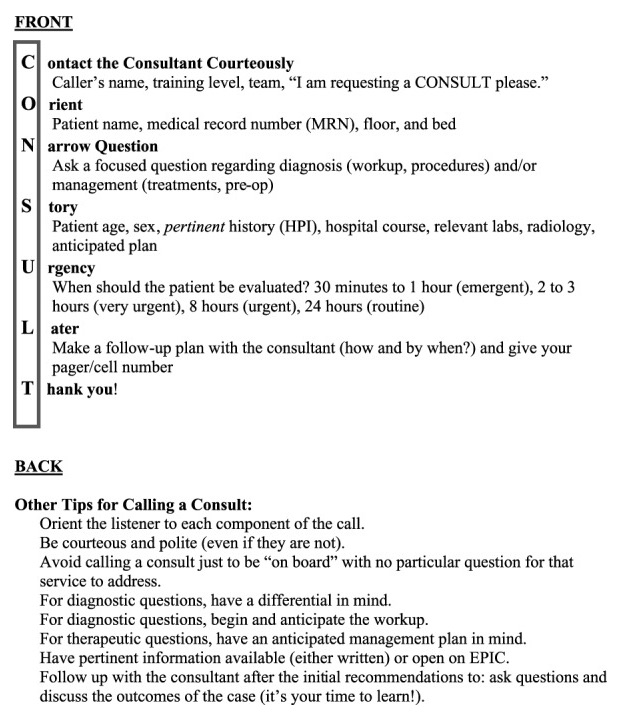
To Call a consult
Introduce yourself, PGY- year, the attending that you are working with and the service that you are on. Say the patient’s name and room number. Give brief PMH and reason for the consult. A mnemonic is included below to summarize the steps and help make your interaction easier. You should only call consults after 8 weeks of training and in the presence of your senior. Once you have finalized your consult call, DON’T FORGET TO PLACE THE CONSULT ORDER ON EPIC!!!
Significant Event Notes & Hospital Courses
- You should write a significant event note or progress note anytime you make a significant intervention in patient care, anytime you evaluate a patient (on nights), anytime there is a Code Blue/Rapid Response called (senior resident can do this as well).
- If present on the note, try to update the hospital course so your colleagues are up to date. This will make your d/c summary so much easier/quicker. This documentation should be CONCISE, and include important information for an outpatient provider to know or for an ED/inpatient provider to know if they are a frequent flyer (i.e. echo results, important changes in long term care).
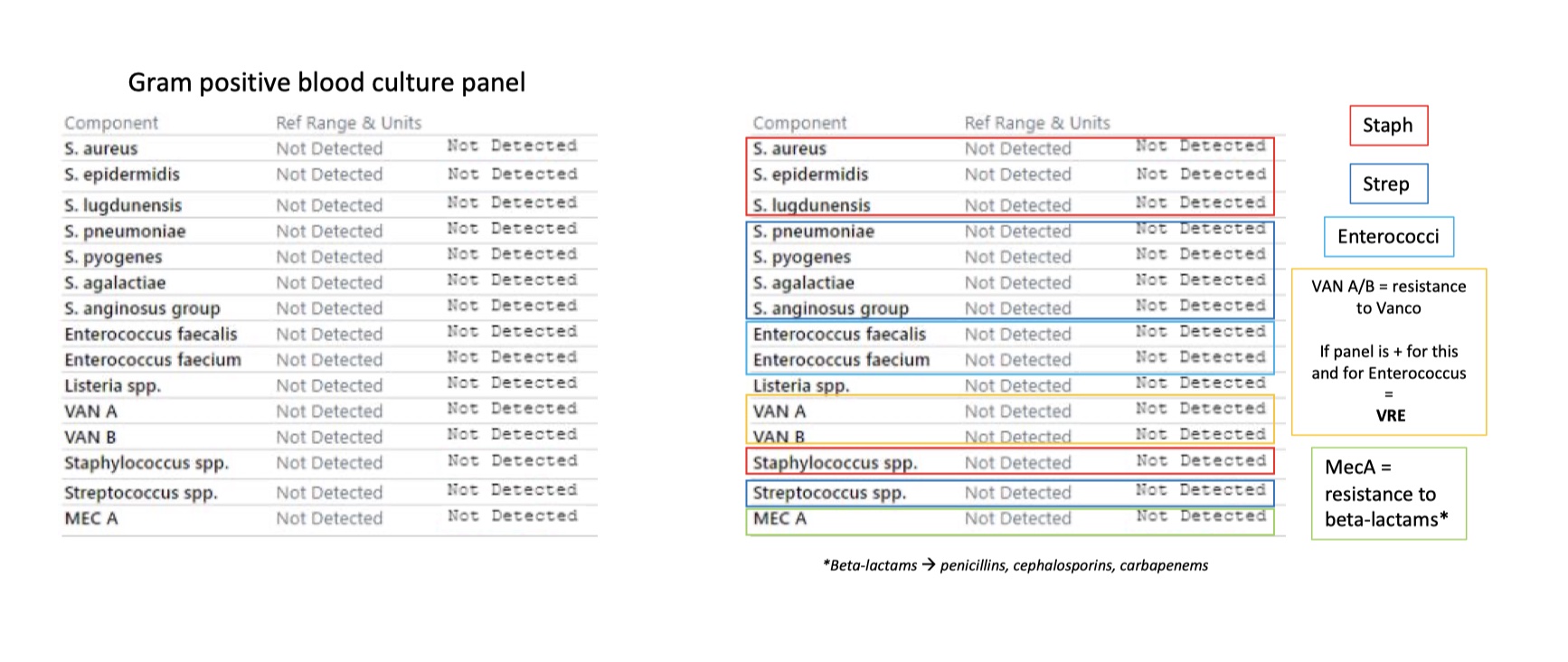
Blood Culture Interpretation
Gram positive blood culture panel interpretations
Gram positive blood culture panel
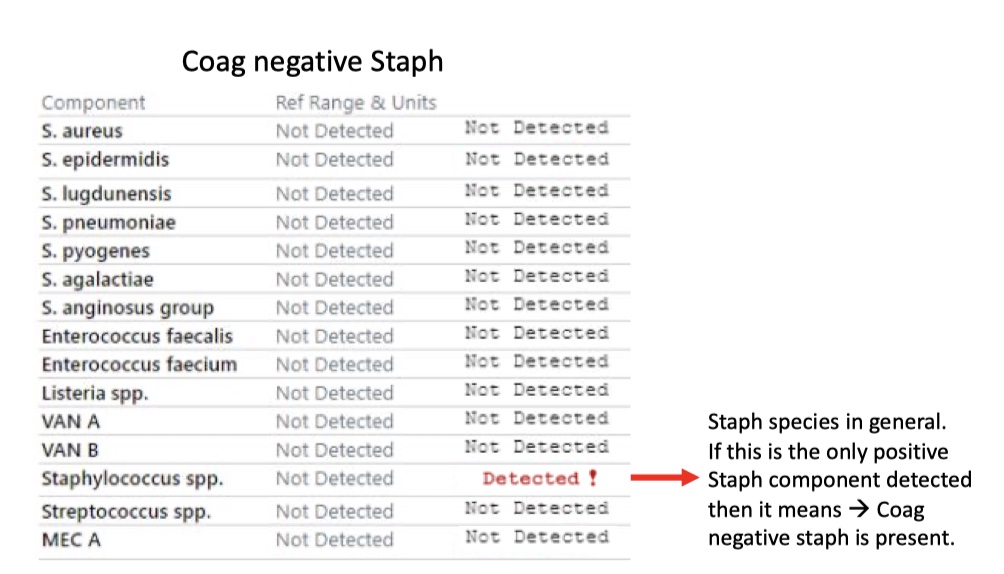
Coag negative Staph
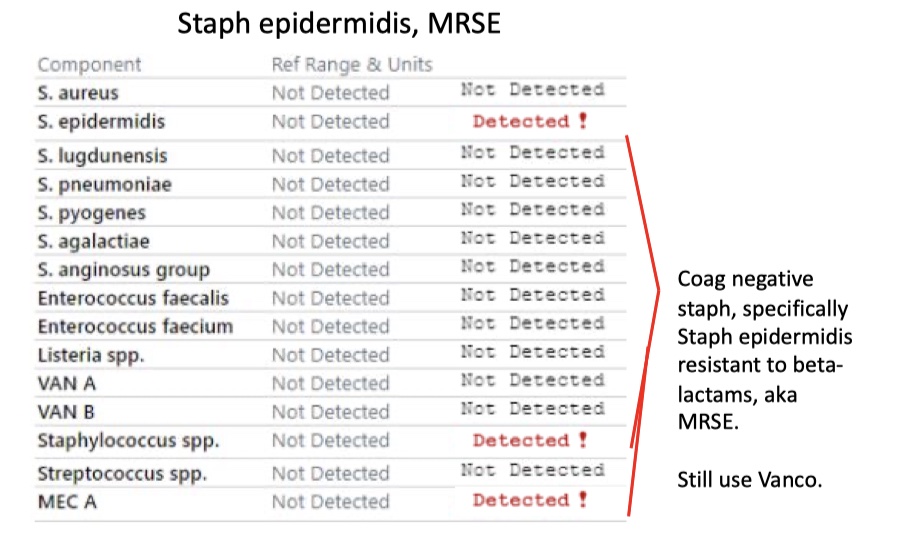
Staph epidermidis, MRSE
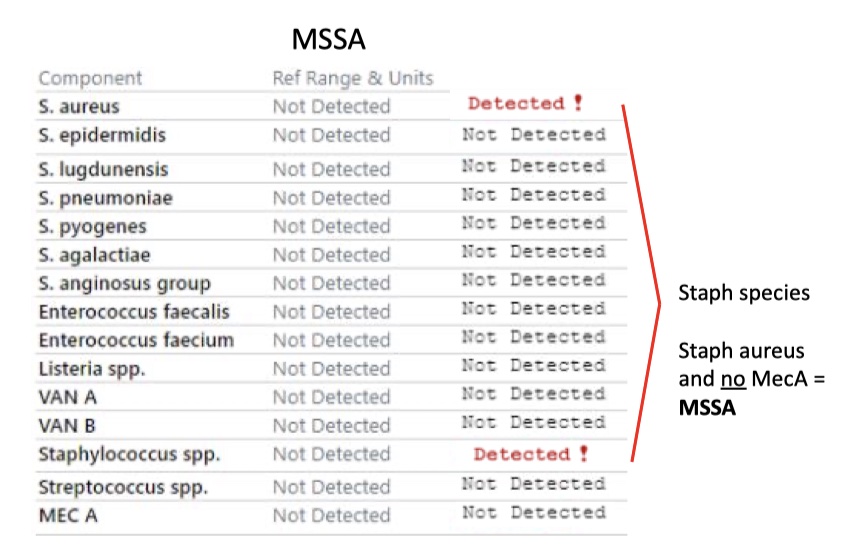
MSSA
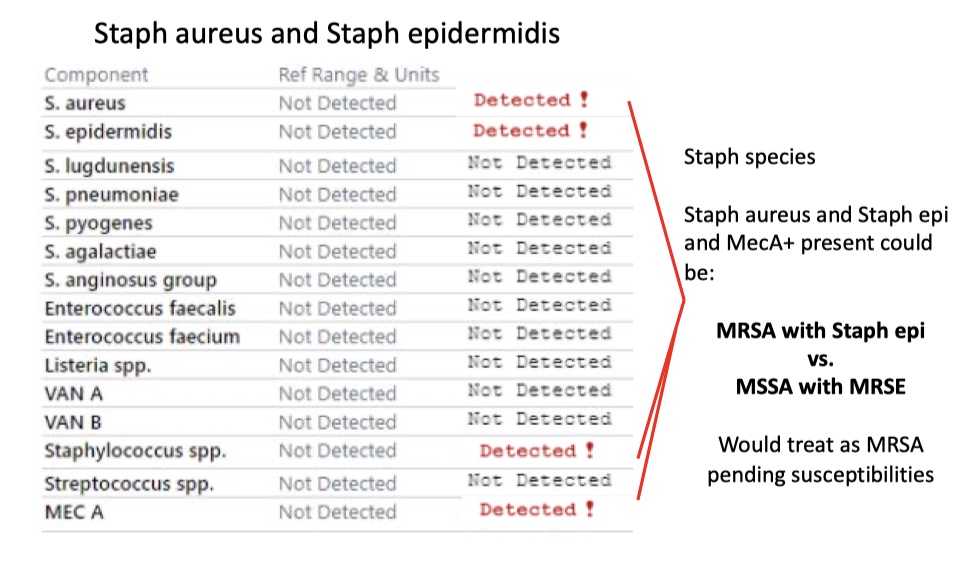
Staph aureus and Staph epidermidis
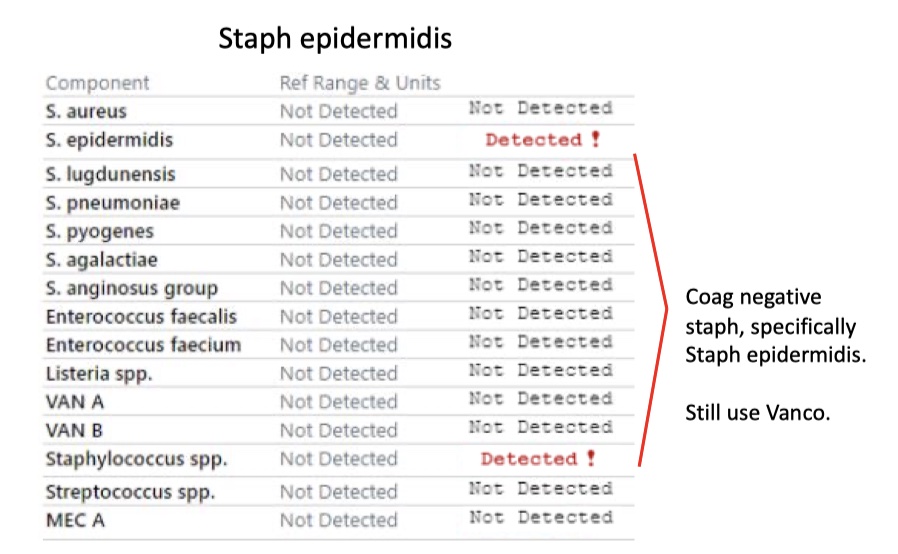
Staph epidermidis
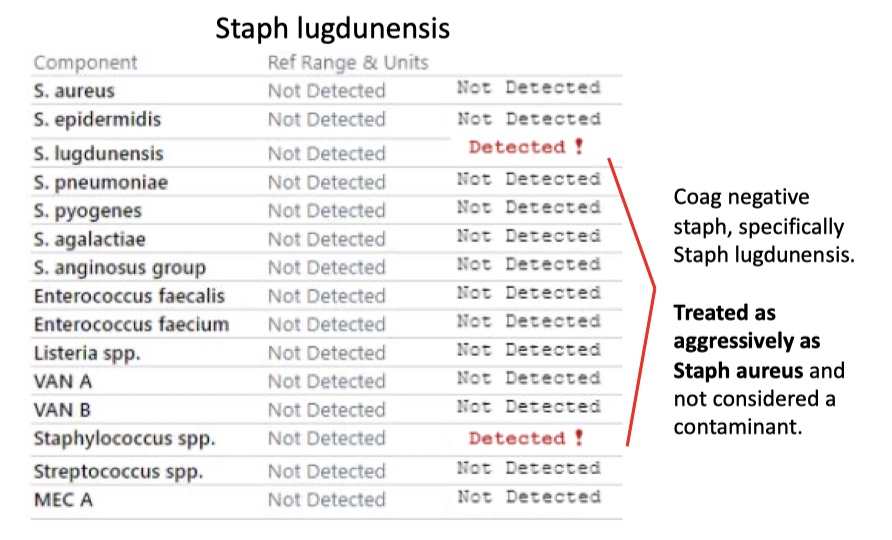
Staph lugdunensis
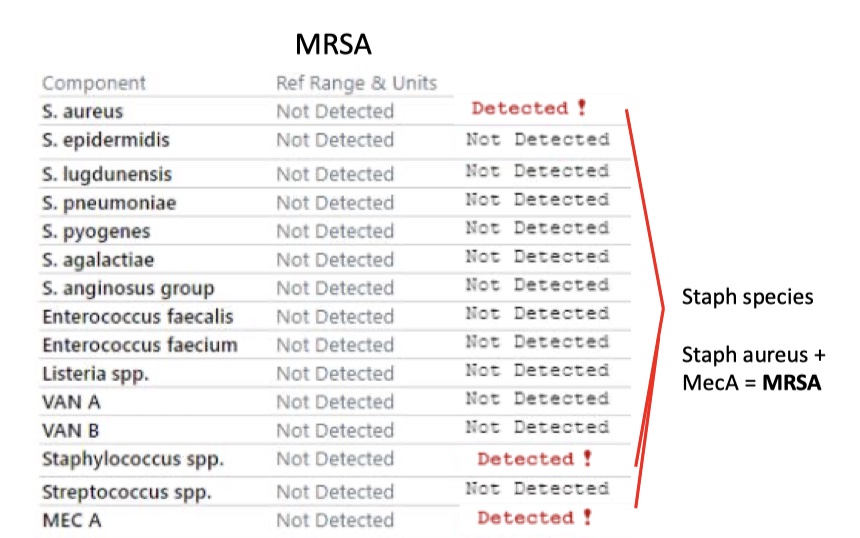
MRSA
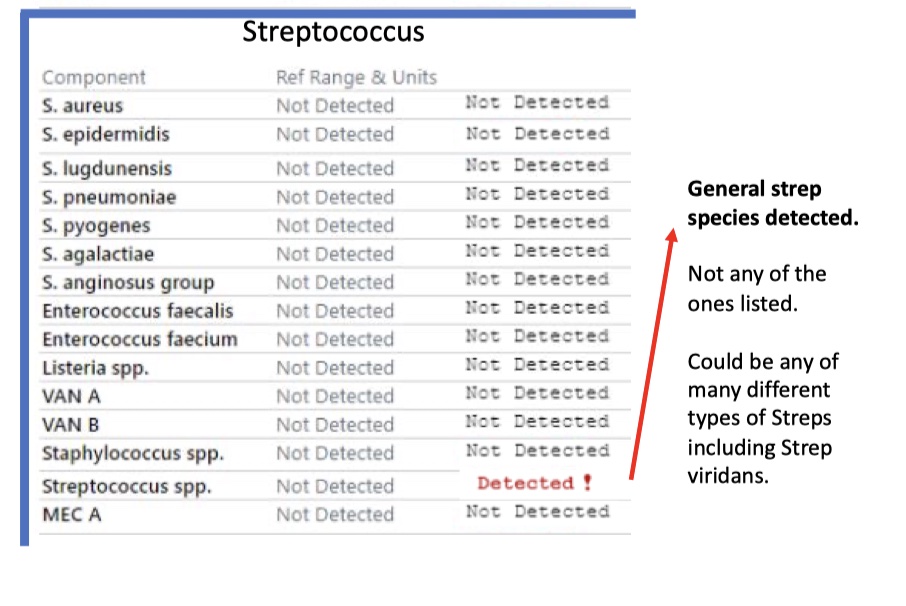
Streptococcus
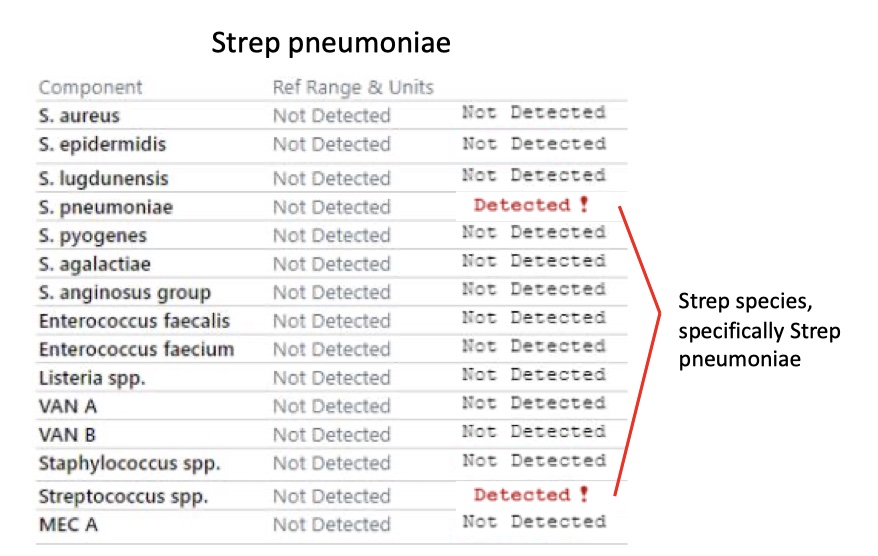
Strep pneumoniae
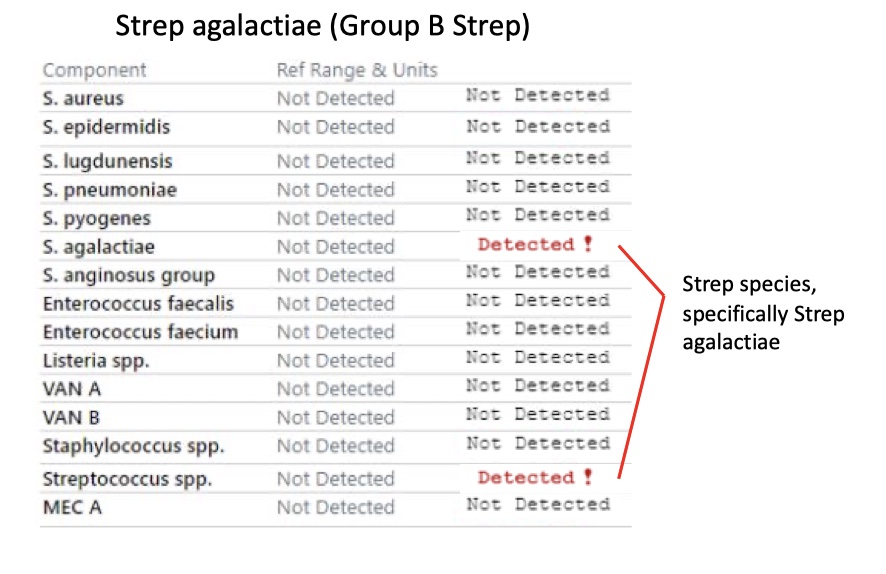
Strep agalactiae (Group B Strep)
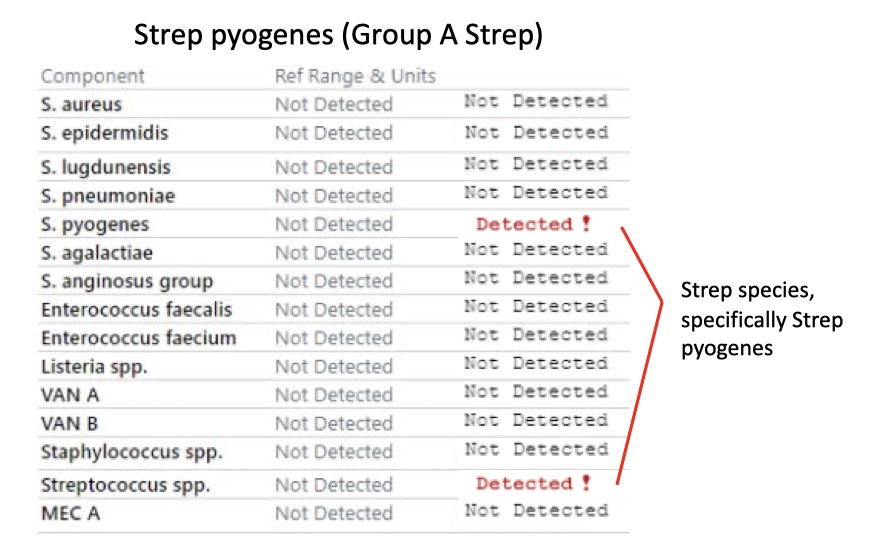
Strep pyogenes (Group A Strep)
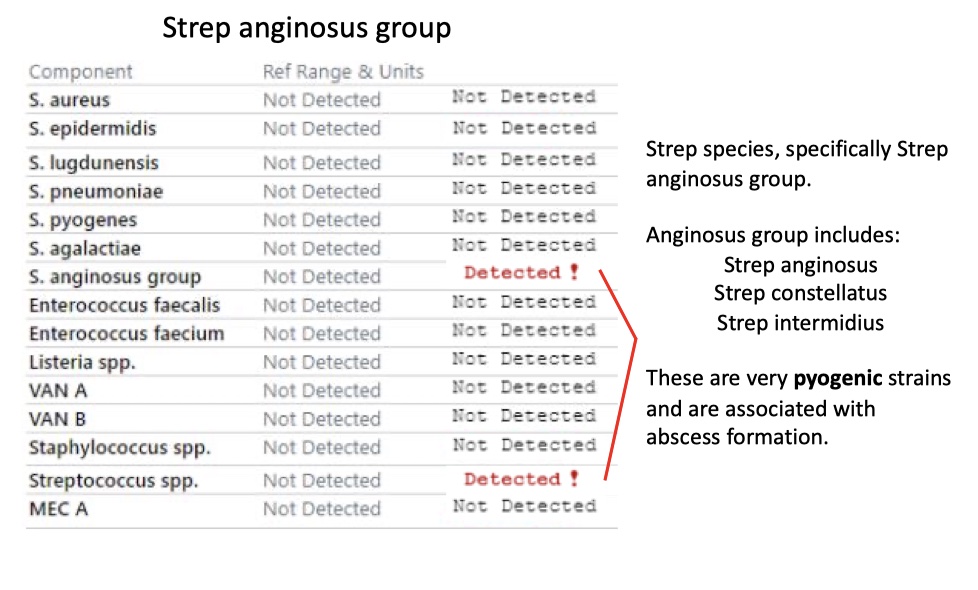
Strep anginosus group
Disclaimer
Always verify with your superiors before taking action based on this guide. The information is intended to help, but not to dictate your course of work. Always use critical judgment and your clinical knowledge skills. This guide will be constantly revised and updated according to evidence-based medicine.