Physical Exam for New Interns
A focused, reliable physical exam is one of the most important skills for interns. It helps you identify clinical changes early, communicate clearly with attendings and consultants, and document findings that support your assessment and plan. The goal is not to perform a full head-to-toe exam on every patient every day, but to perform a thoughtful exam based on the patient's chief complaint, active problems, and overnight events.
General Approach
Before entering the room, briefly review the patient's diagnosis, vitals, overnight events, labs, imaging, oxygen requirement, and current treatment plan. This helps you know what findings to look for.
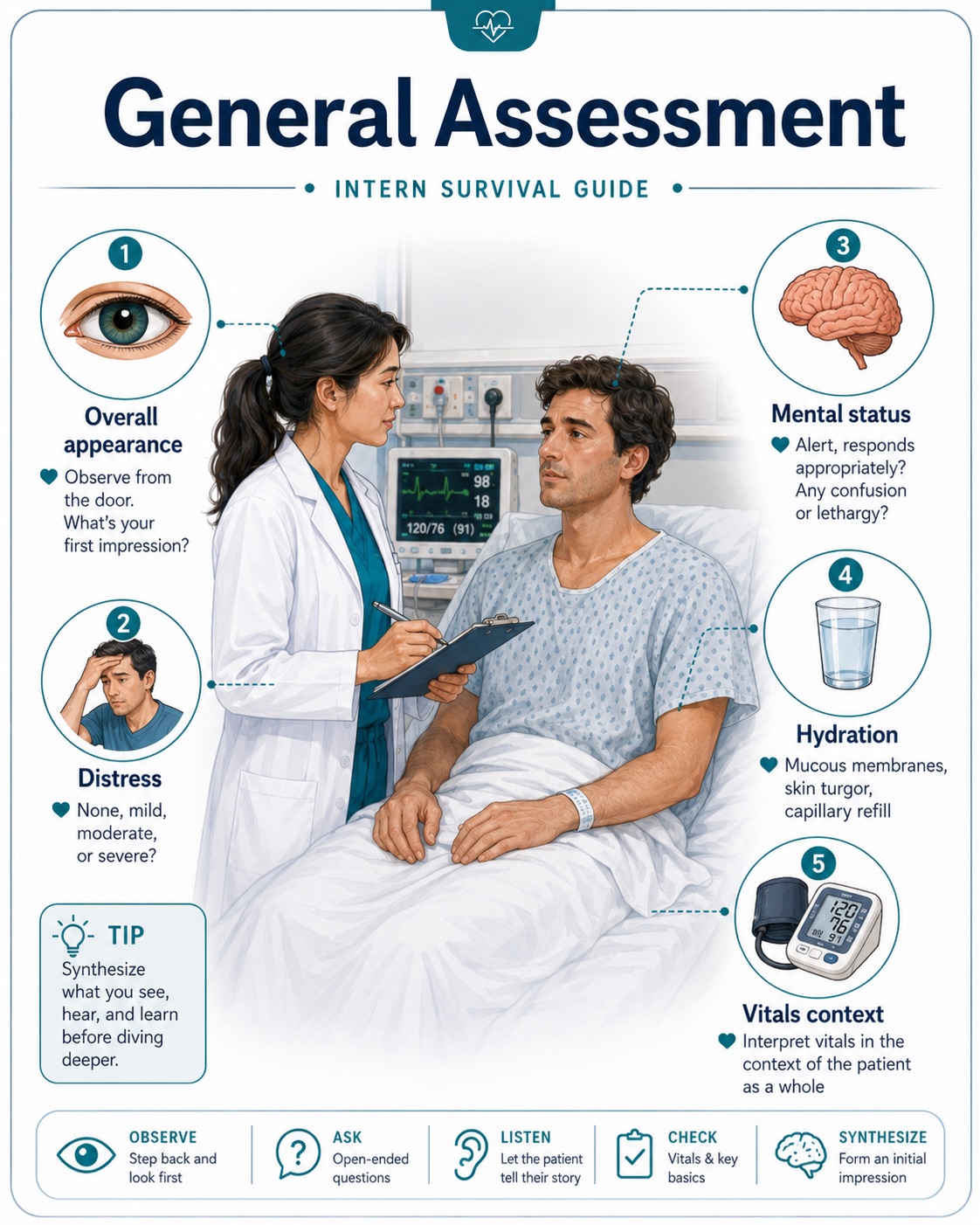
Always start with the patient's overall appearance. Ask yourself: Does the patient look comfortable or toxic? Are they in distress? Are they awake, confused, lethargic, or agitated? Are they breathing comfortably? Are they able to speak in full sentences?
The One Question Every Daily Exam Should Answer
"Is this patient better, worse, or unchanged compared with yesterday?"
Basic Daily Physical Exam Template
General: Alert and oriented, no acute distress, appears comfortable/uncomfortable, ill-appearing, toxic-appearing, or lethargic.
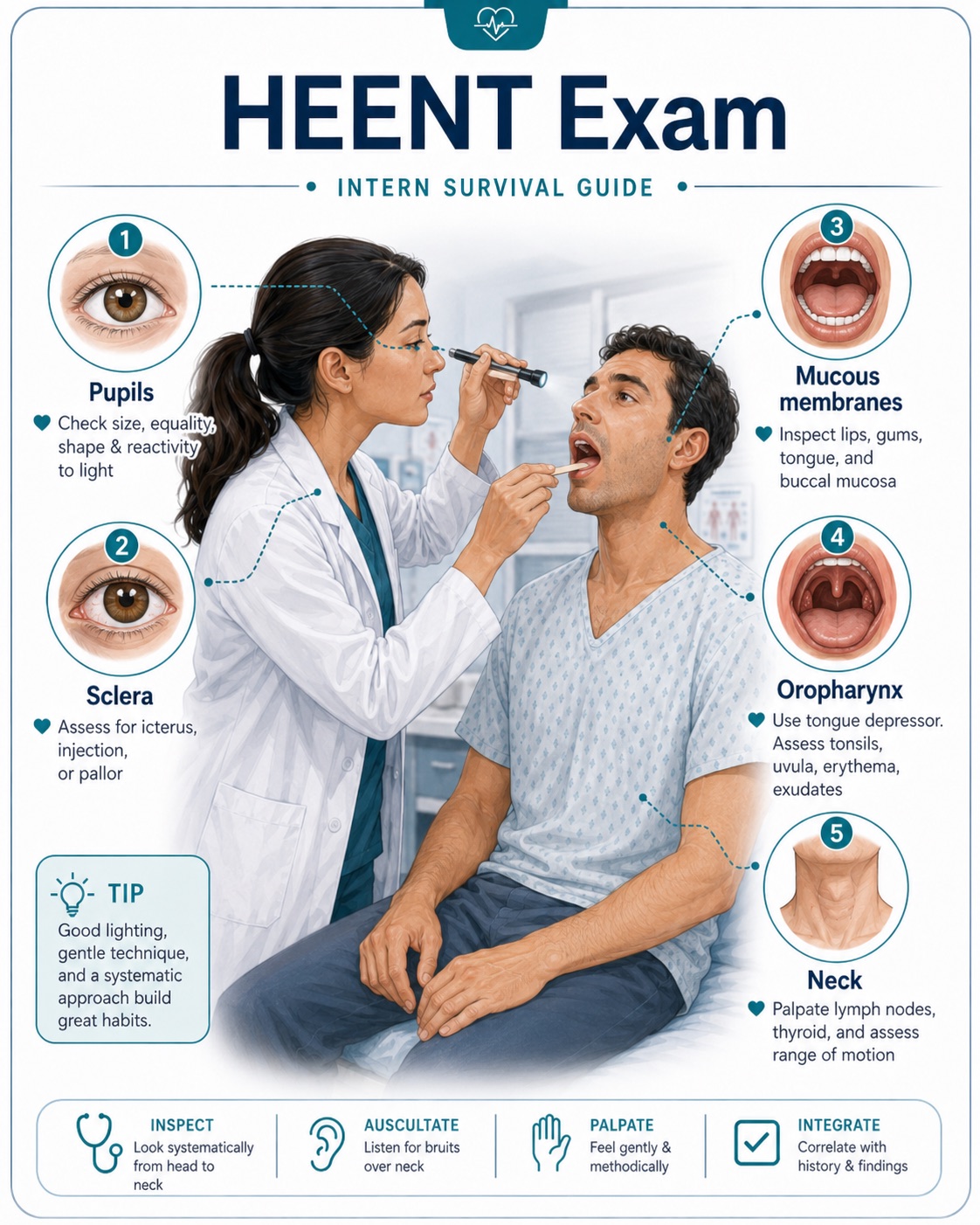
HEENT: Normocephalic, atraumatic. Pupils equal and reactive if relevant. Mucous membranes moist or dry. No scleral icterus.
Cardiovascular: Regular rate and rhythm. No murmurs, rubs, or gallops. Peripheral pulses intact. Assess for JVD and lower extremity edema when evaluating volume status or heart failure.

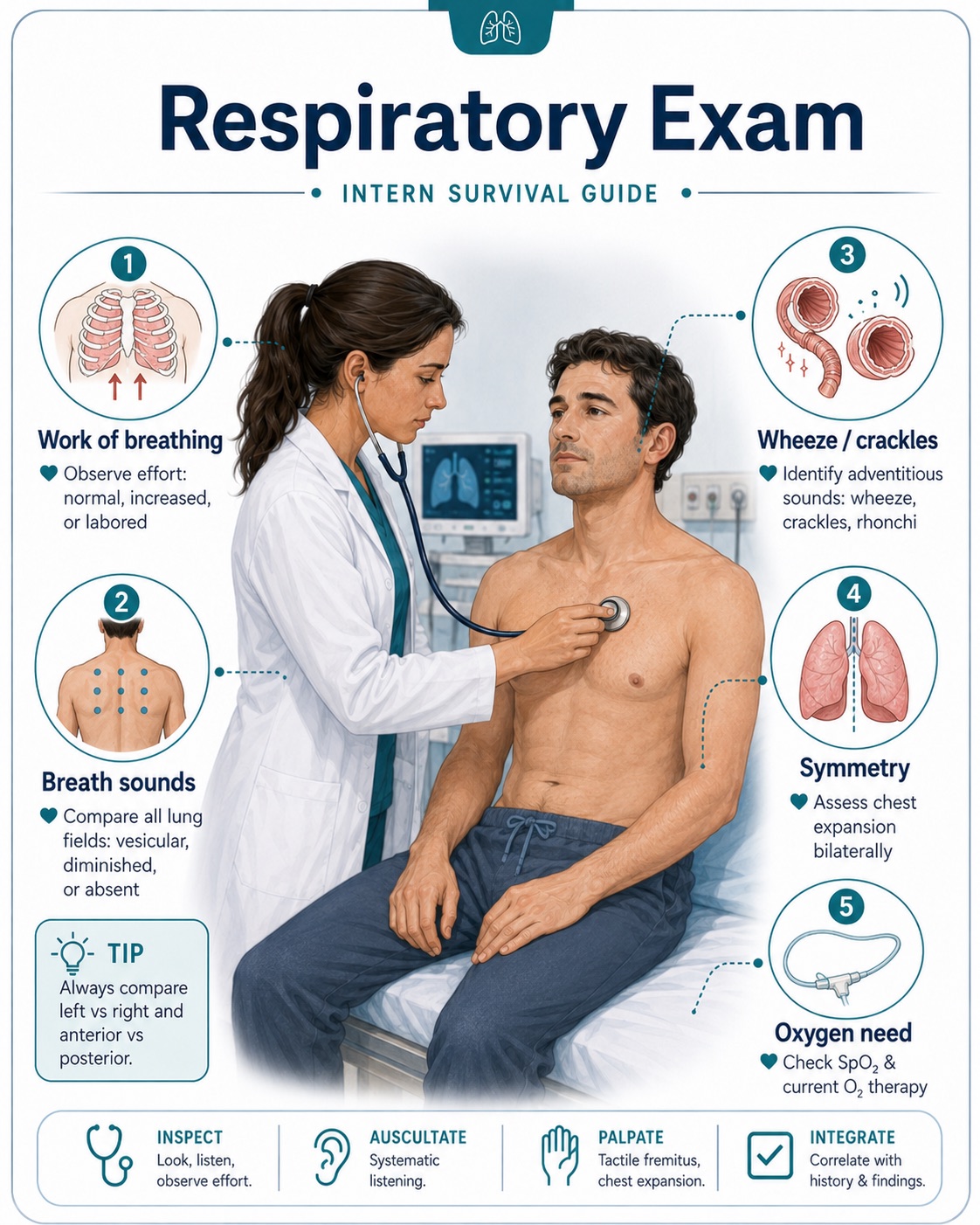
Respiratory: Normal work of breathing. Clear to auscultation bilaterally, or note wheezing, crackles, rhonchi, diminished breath sounds, accessory muscle use, or oxygen requirement.
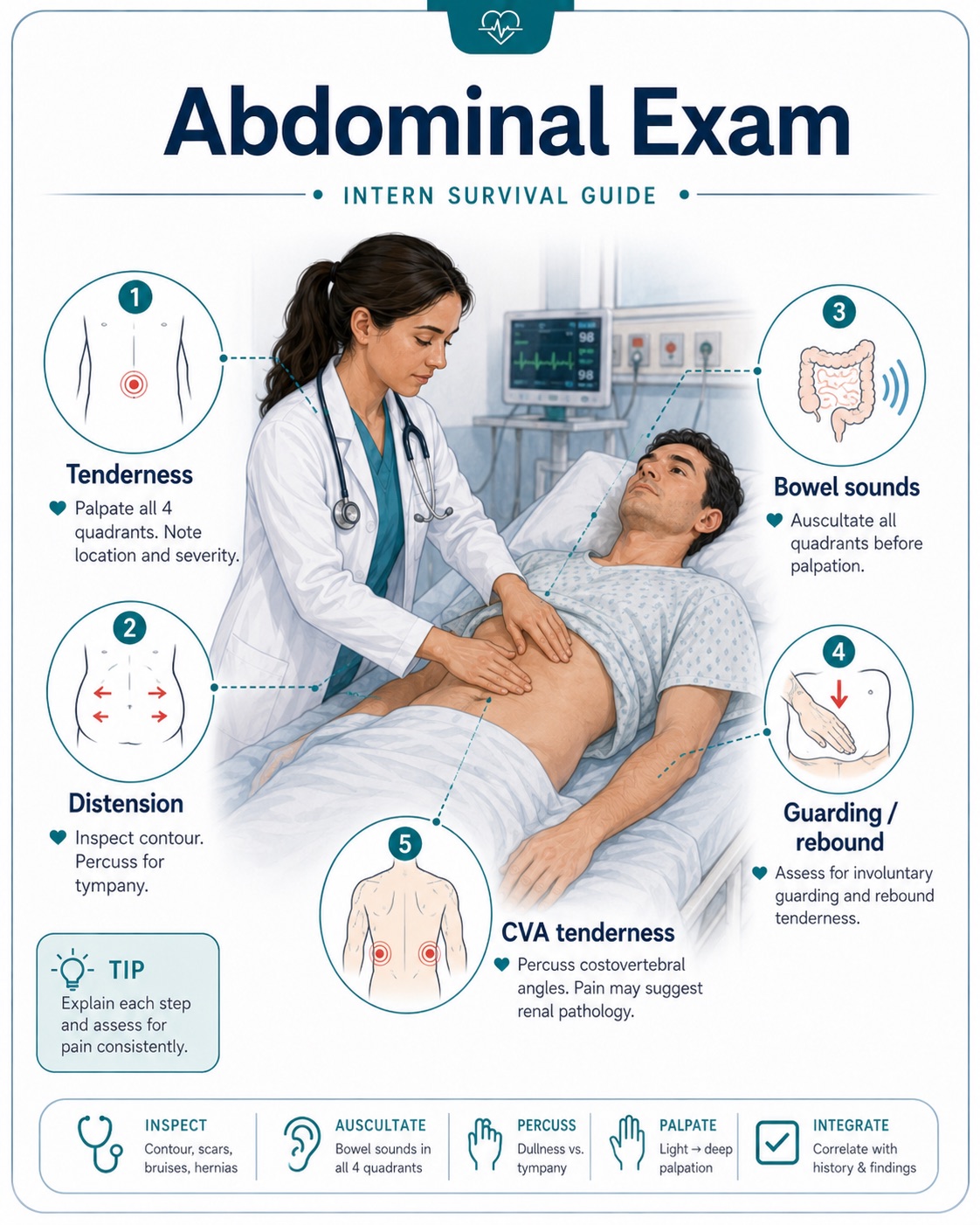
Abdomen: Soft, non-distended, non-tender. Bowel sounds present. Note guarding, rebound, rigidity, suprapubic tenderness, or CVA tenderness when relevant.
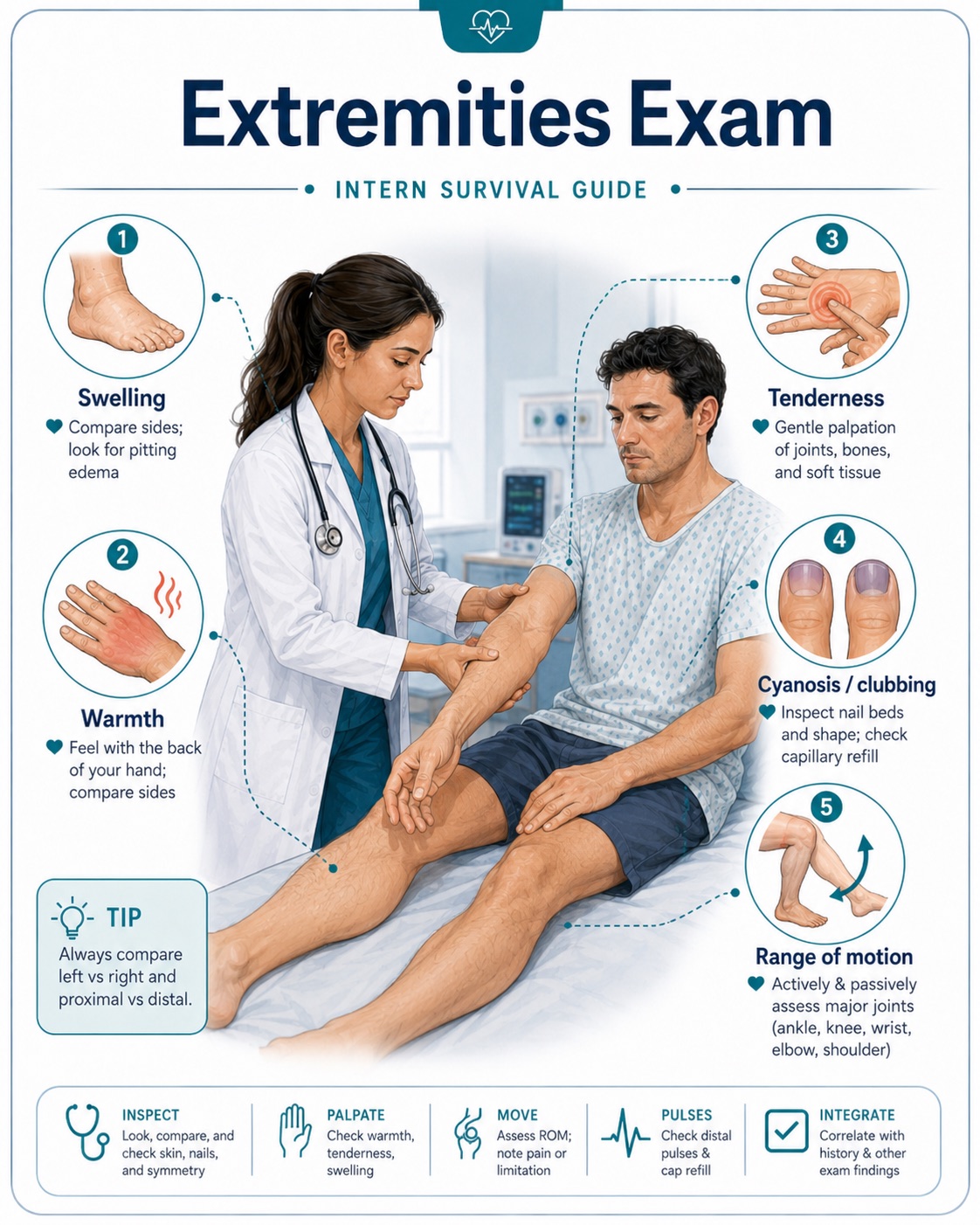
Extremities: No edema, cyanosis, or clubbing. Assess tenderness, erythema, warmth, swelling, range of motion, and pulses when indicated.
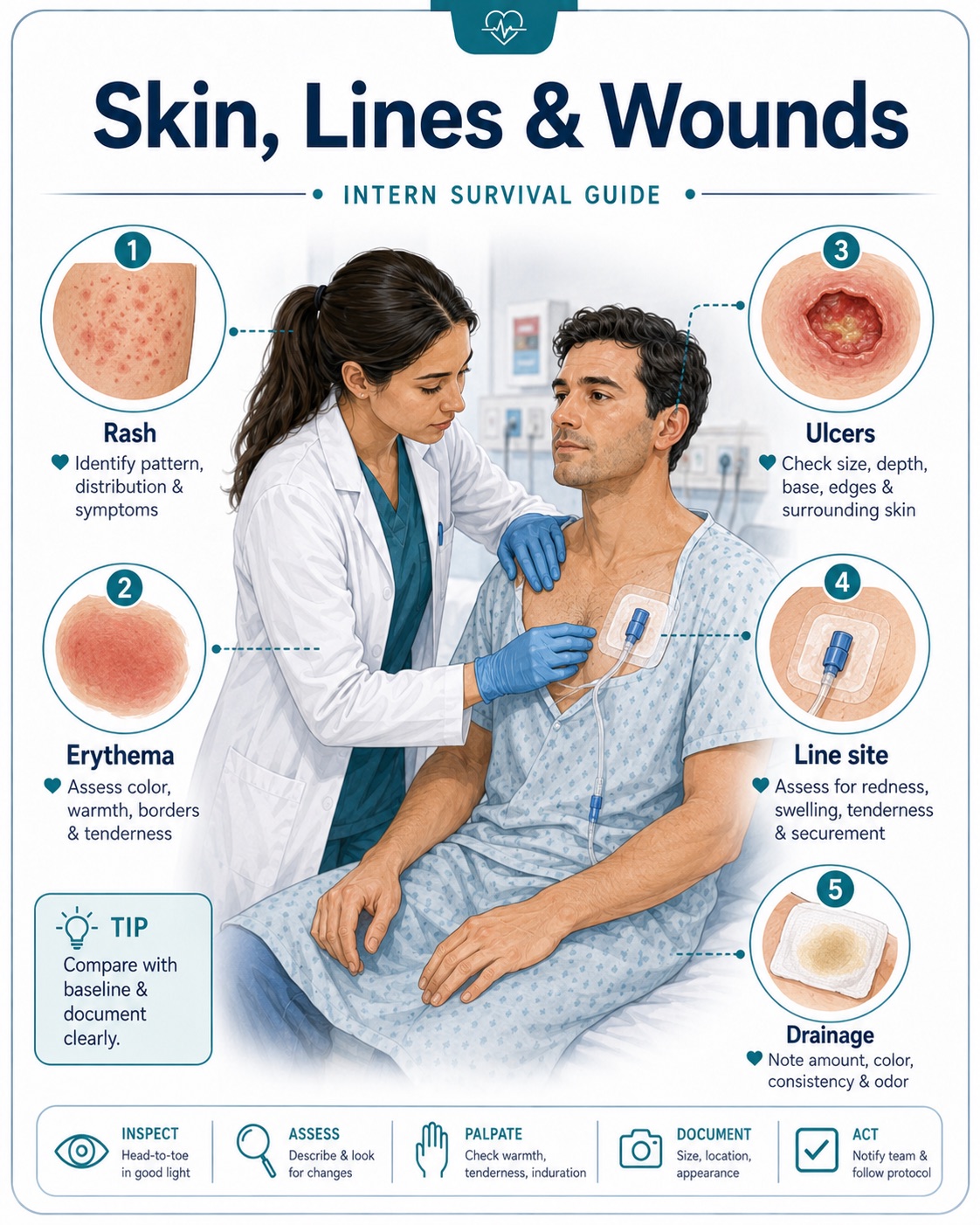
Skin: Warm and dry. No rash, wounds, ulcers, cellulitis, bruising, or pressure injuries. Examine lines, drains, and surgical sites when present.
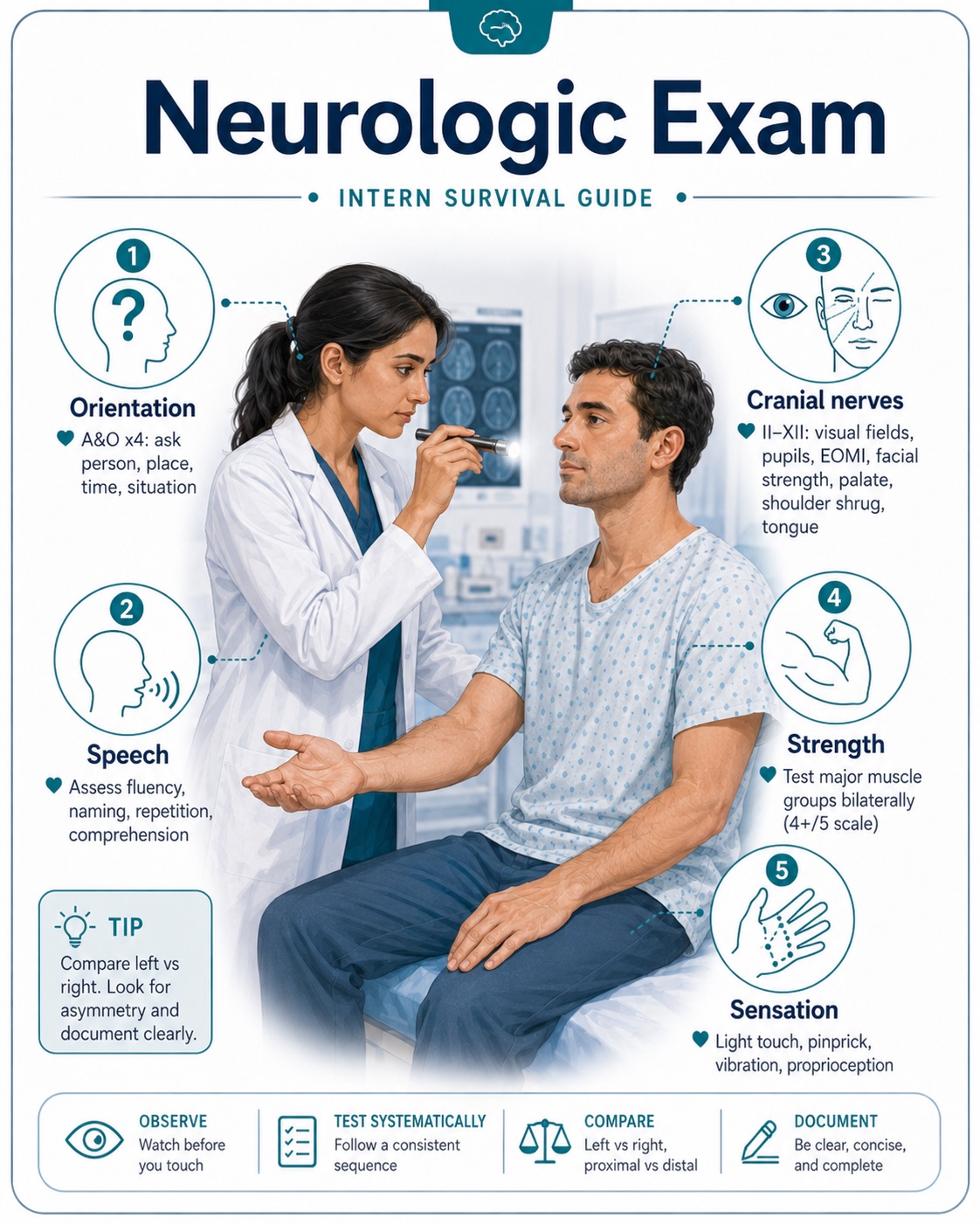
Neurologic: Awake and oriented. No focal deficits. Strength and sensation grossly intact. Cranial nerves, pronator drift, speech, gait, or cerebellar testing if stroke, weakness, dizziness, or altered mental status is a concern.
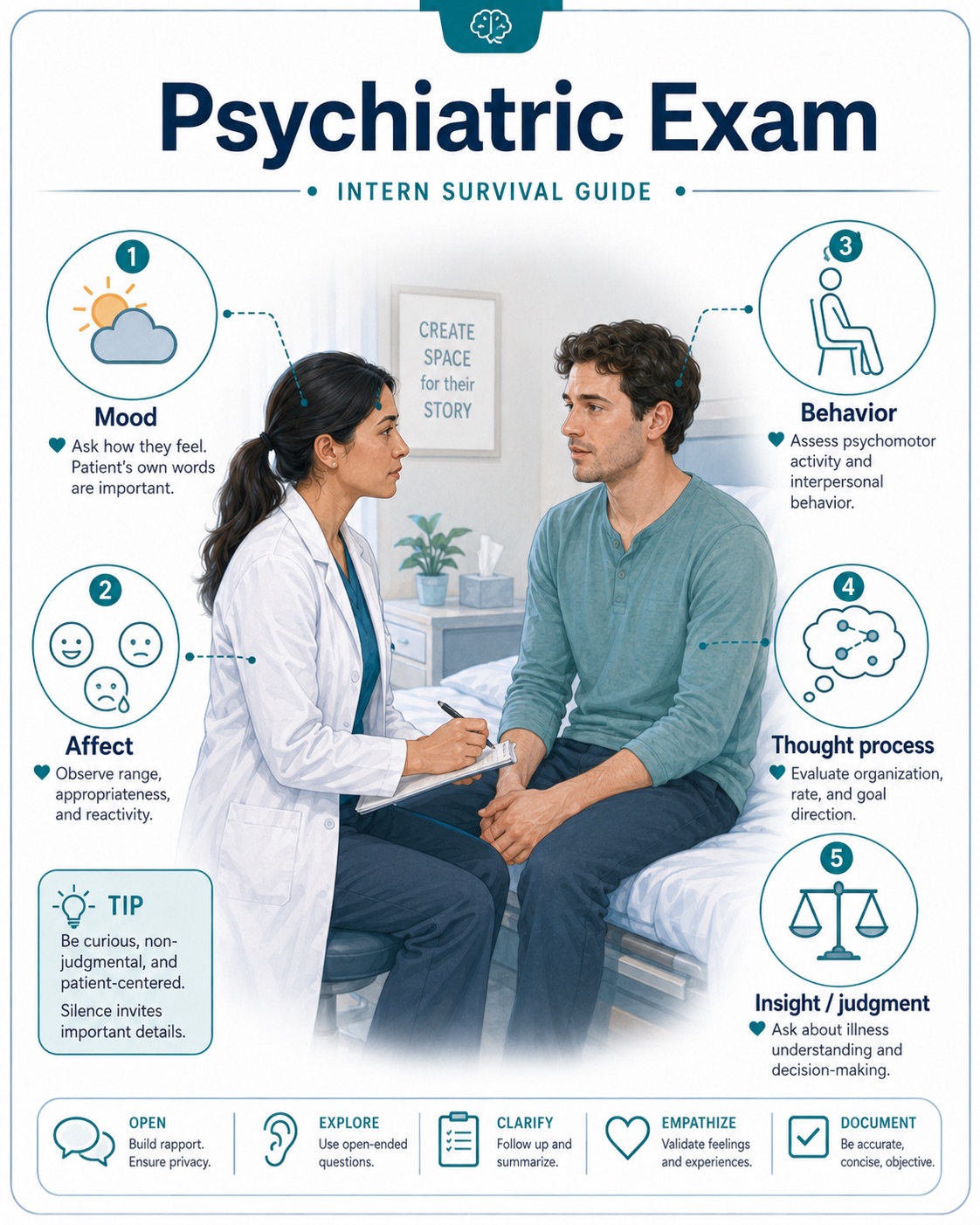
Psychiatric: Appropriate mood and affect. Cooperative, anxious, agitated, confused, or withdrawn when clinically relevant.
High-Yield Exam Findings by System
Cardiovascular
For chest pain, heart failure, syncope, arrhythmias, or shock, focus on:
- Heart rate and rhythm
- Murmurs, especially new systolic murmur
- JVD
- Peripheral edema
- Peripheral pulses
- Capillary refill and extremity temperature
- Signs of volume overload or poor perfusion
Useful documentation examples:
- "Regular rate and rhythm, no murmurs, no JVD, no bilateral lower extremity edema."
- "Irregularly irregular rhythm, tachycardic, 2+ bilateral lower extremity edema, mild JVD."
- "Extremities cool to touch with delayed capillary refill, concerning for poor perfusion."
Respiratory
For shortness of breath, pneumonia, COPD/asthma, CHF, hypoxia, or PE concern, assess:
- Work of breathing
- Ability to speak in full sentences
- Oxygen requirement
- Crackles, wheezing, rhonchi, or diminished breath sounds
- Accessory muscle use
- Symmetry of breath sounds
Useful documentation examples:
- "Normal work of breathing on room air, lungs clear to auscultation bilaterally."
- "Diffuse bilateral expiratory wheezing with prolonged expiratory phase."
- "Bibasilar crackles with decreased breath sounds at the right lung base."
- "Increased work of breathing with accessory muscle use, requiring 4 L nasal cannula."
Abdomen
For abdominal pain, GI bleed, pancreatitis, obstruction, urinary symptoms, or sepsis, assess:
- Tenderness location
- Distension
- Guarding, rebound, or rigidity
- Bowel sounds
- CVA tenderness
- Suprapubic tenderness
- Surgical scars, drains, PEG tube, ostomy, or wounds
Useful documentation examples:
- "Abdomen soft, non-distended, mild epigastric tenderness, no rebound or guarding."
- "Diffuse abdominal tenderness with voluntary guarding, no rigidity."
- "Left CVA tenderness present."
- "Suprapubic tenderness present, no rebound or guarding."
Neurologic
For altered mental status, stroke symptoms, falls, dizziness, weakness, or seizures, assess:
- Alertness and orientation
- Speech
- Pupils
- Facial symmetry
- Strength in all extremities
- Sensation
- Pronator drift
- Coordination if relevant
- Gait if safe
Useful documentation examples:
- "Alert and oriented x3, speech clear, no facial droop, strength 5/5 in all extremities, sensation intact."
- "Confused but awake, oriented to self only, follows simple commands, no obvious focal motor deficit."
- "Right-sided facial droop with 4/5 strength in right upper and lower extremities."
Musculoskeletal
The musculoskeletal exam is especially important for patients presenting with falls, joint pain, back pain, weakness, trauma, inability to ambulate, cellulitis vs. septic arthritis, gout, or functional decline. Assess:
- Pain location and severity
- Joint swelling, erythema, warmth, or deformity
- Range of motion, both active and passive if tolerated
- Tenderness to palpation
- Strength in major muscle groups
- Gait and ability to bear weight, if safe
- Spine tenderness, especially after falls or trauma
- Signs of inflammatory arthritis, gout, septic arthritis, or fracture
Useful documentation examples:
- "Normal range of motion in bilateral upper and lower extremities. No joint swelling, erythema, warmth, or deformity."
- "Right knee with mild swelling and tenderness to palpation, no erythema or warmth. Range of motion limited due to pain."
- "Left hip tender to palpation with limited range of motion due to pain. Patient unable to bear weight."
- "Midline lumbar spine tenderness present. No obvious step-off or deformity."
- "Bilateral knees with chronic osteoarthritic changes, no acute swelling, erythema, or warmth."
Don't Miss Septic Arthritis
For suspected septic arthritis, carefully document whether the joint is warm, swollen, and erythematous, and whether passive range of motion is painful. A hot, swollen joint with severe pain on passive range of motion should prompt urgent evaluation.
Skin, Lines, and Wounds
Do not forget to examine lines, wounds, and devices. These are common sources of infection and complications. Check:
- Peripheral IV sites
- PICC lines and central lines
- Foley catheter
- Surgical incisions
- Pressure injuries
- Diabetic foot wounds
- Drain sites
- PEG/trach sites
Useful documentation examples:
- "PICC line site clean, dry, and intact without erythema or drainage."
- "Sacral pressure injury noted with surrounding erythema, no purulent drainage."
- "Right foot ulcer with surrounding warmth and erythema, no crepitus."
Exam Tips for Interns
- Document only what you actually examined. Avoid copying forward an exam that was not performed.
- Compare with prior exams. If crackles, edema, confusion, weakness, or abdominal tenderness are improving or worsening, mention the trend.
- Use specific language. Instead of "normal neuro exam," write the key findings: orientation, speech, strength, facial symmetry, and focal deficits.
- Always reassess patients with clinical changes. New fever, hypotension, tachycardia, hypoxia, chest pain, altered mental status, abdominal pain, or a fall should prompt a bedside exam.
- For unstable patients, start with ABCs: airway, breathing, circulation. Check mental status, vitals, oxygen requirement, work of breathing, pulses, perfusion, and signs of shock.
Focused Exam Examples
Chest Pain
General appearance, vitals, cardiac exam, lung exam, chest wall tenderness, pulses, lower extremity edema, signs of DVT if PE is considered.
"Patient comfortable, no acute distress. Regular rate and rhythm, no murmurs. Lungs clear bilaterally. No chest wall tenderness. No lower extremity edema or calf tenderness."
Shortness of Breath
Work of breathing, oxygen requirement, lung sounds, JVD, edema, heart rhythm, mental status.
"Mild increased work of breathing on 3 L nasal cannula. Bibasilar crackles present. Mild JVD and 1+ bilateral lower extremity edema."
Abdominal Pain
Pain location, distension, bowel sounds, rebound, guarding, rigidity, CVA tenderness, suprapubic tenderness.
"Abdomen soft, mildly distended, tender to palpation in right lower quadrant, no rebound or guarding."
Altered Mental Status
Orientation, attention, speech, pupils, facial droop, strength, sensation, signs of infection, respiratory status, medication/sedation effects.
"Awake but confused, oriented to self only. Speech fluent. No facial droop. Moves all extremities spontaneously. No focal neurologic deficit appreciated."
Fall
Head trauma, neck/back pain, focal neuro deficits, extremity pain, range of motion, gait if safe, anticoagulation status.
"Patient evaluated after fall. No visible head trauma. No cervical spine tenderness. Alert and oriented x3. No focal neurologic deficits. Full range of motion of bilateral upper and lower extremities without deformity."
Volume Status
Volume assessment is very common but can be difficult. Look for mucous membranes, skin turgor, JVD, lung crackles, peripheral edema, daily weight, intake/output, blood pressure and heart rate trends, creatinine/BUN trend, and response to fluids or diuretics.
"Exam concerning for volume overload with bibasilar crackles, elevated JVD, and 2+ bilateral lower extremity edema."
"Appears volume depleted with dry mucous membranes, tachycardia, and poor oral intake."
Sepsis Concern
General appearance, mental status, perfusion, capillary refill, skin temperature, lung exam, abdominal exam, CVA tenderness, lines/wounds.
"Ill-appearing and febrile. Tachycardic. Extremities warm with intact pulses. Lungs with right basilar crackles. Abdomen soft and non-tender. No CVA tenderness. PICC site without erythema or drainage."
Final Reminder
A strong physical exam does not need to be long. It needs to be accurate, focused, and clinically useful. When in doubt, go to bedside, examine the patient yourself, and document what changed.
 Contributed by Mafaz Mansoor, MD
Contributed by Mafaz Mansoor, MD